Semaglutide therapy decreases epicardial fat inflammation and improves psoriasis severity in patients affected by abdominal obesity and type-2 diabetes
- PMID: 37551923
- PMCID: PMC10448542
- DOI: 10.1530/EDM-23-0017
Semaglutide therapy decreases epicardial fat inflammation and improves psoriasis severity in patients affected by abdominal obesity and type-2 diabetes
Abstract
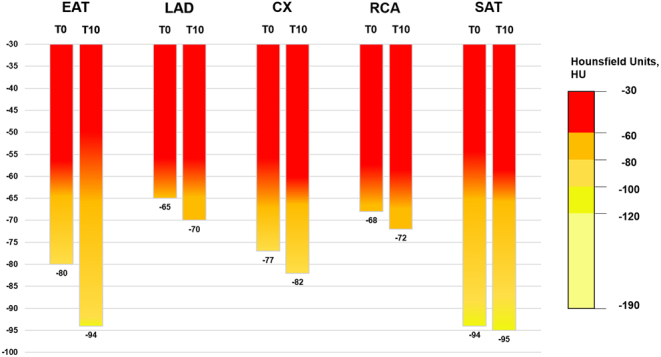
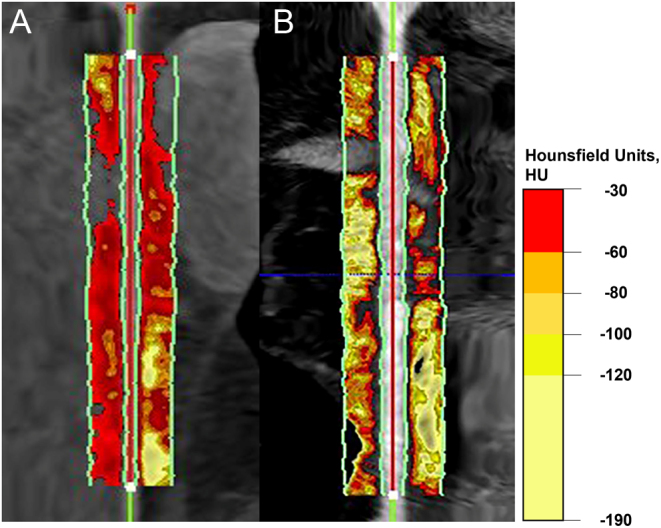
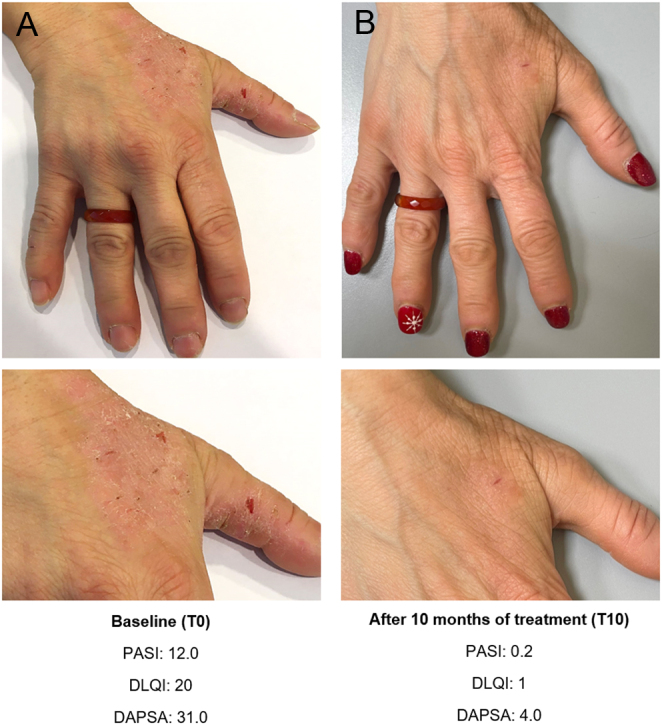
Summary: Psoriasis is often associated with abdominal obesity and type-2 diabetes (T2D). The inflammatory process in psoriasis can target adipose tissue depots, especially those surrounding the heart and coronary arteries, exposing to an increased risk of cardiovascular diseases. A 50-year-old female patient referred to us for abdominal obesity and T2D, which were not controlled with lifestyle modifications. She had suffered from psoriasis for some years and was treated with guselkumab, without success. Epicardial adipose tissue (EAT) attenuation and pericoronary adipose tissue (PCAT) attenuation for each coronary, defined as mean attenuation expressed in Hounsfield unit (HU), were assessed by routine coronary computed tomography angiography. At baseline, EAT attenuation was -80 HU and PCAT attenuation of the right coronary artery (RCA) was -68 HU, values associated with an increased cardiac mortality risk. Psoriasis area and severity index (PASI) was 12.0, indicating severe psoriasis, while dermatology life quality index (DLQI) was 20, indicating a negative effect on the patient's life. Semaglutide (starting with 0.25 mg/week for 4 weeks, increased to 0.50 mg/week for 16 weeks, and then to 1 mg/week) was started. After 10 months, semaglutide treatment normalized glycated hemoglobin and induced weight loss, particularly at abdominal level, also followed by a reduction in computed tomography-measured EAT volume. EAT attenuation and PCAT attenuation of RCA decreased, showing an important reduction of 17.5 and 5.9% respectively, compared with baseline. PASI and DLQI decreased by 98.3 and 95% respectively, indicating an improvement in psoriasis skin lesions and an important amelioration of the patient's quality of life, compared with baseline.
Learning points: Psoriasis patients affected by obesity and type-2 diabetes (T2D) are often resistant to biologic therapies. Psoriasis is often associated with abdominal obesity, T2D, and cardiovascular diseases (CVD), given their shared inflammatory properties and pathogenic similarities. Epicardial adipose tissue (EAT) inflammation can cause the distinctive pattern of CVD seen in psoriasis. EAT and pericoronary adipose tissue (PCAT) attenuation, assessed by routine coronary computed tomography angiography (CCTA), can be used as biomarkers of inflammation and allow monitoring of medical anti-inflammatory therapies. The actions of semaglutide to reduce energy intake, improve glycemic control, and produce effective weight loss, particularly at the visceral fat depot level, can diminish adipose tissue dysfunction, reduce EAT attenuation and PCAT attenuation of the right coronary artery (RCA) and concomitantly ameliorate the clinical severity of psoriasis. Semaglutide therapy may be considered in psoriasis patients affected by T2D and abdominal obesity, despite low cardiovascular risk by traditional risk scores, who are resistant to biologic therapies.
Conflict of interest statement
There is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Figures