

The addition of rituximab to chemotherapy improves overall survival in mantle cell lymphoma-a pooled trials analysis
- PMID: 37552322
- PMCID: PMC10492741
- DOI: 10.1007/s00277-023-05385-1
The addition of rituximab to chemotherapy improves overall survival in mantle cell lymphoma-a pooled trials analysis
Abstract
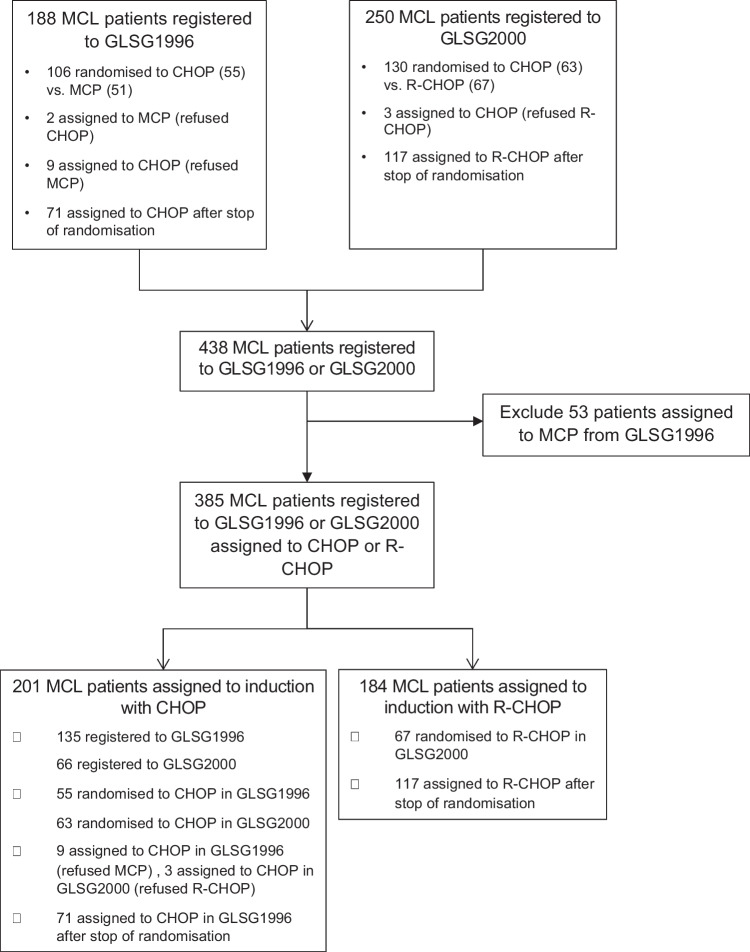
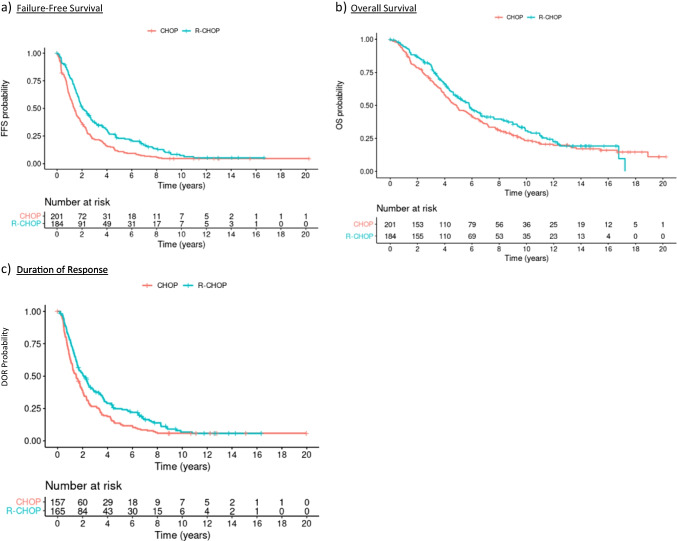
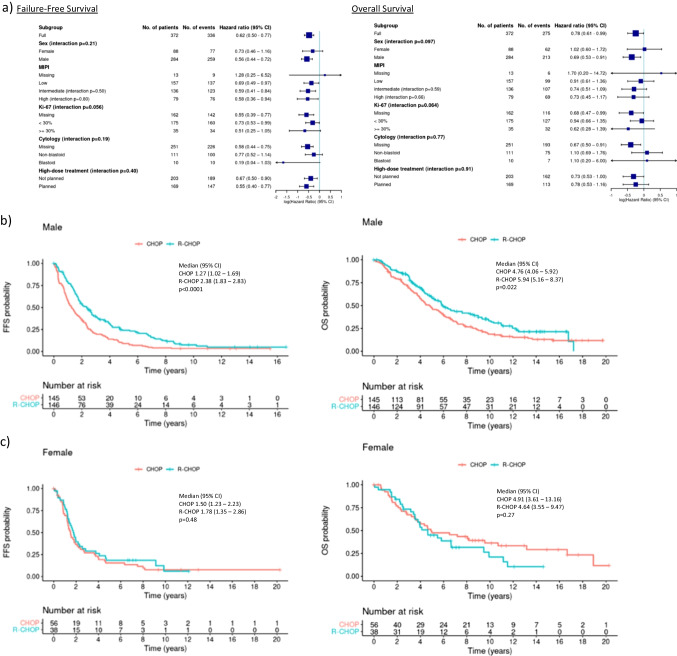
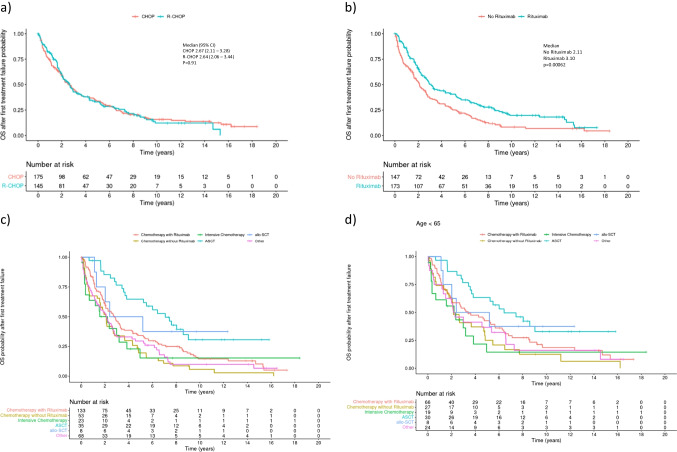
Mantle cell lymphoma (MCL) is a distinct subtype of B-cell lymphoma and commonly used induction immunochemotherapies include the anti-CD20 antibody rituximab. However, efficacy data for rituximab regarding overall survival (OS) in first line MCL therapy remain conflicting.We report long-term outcomes of a pooled trials analysis comparing Cyclophosphamide, Doxorubicine, Vincristine, Prednisone (CHOP) to R-CHOP in MCL to confirm efficacy on failure free survival (FFS) and OS in relevant subgroups. Untreated, adult MCL patients of two prospective trials assigned to CHOP or R-CHOP were included. Primary endpoints were FFS and OS, secondary endpoints included duration of response (DOR), secondary malignancies and OS after relapse. Between 1996 and 2003, 385 MCL patients were assigned to CHOP (201) or R-CHOP (184). After a median follow-up of 13.4 years, the addition of Rituximab significantly improved FFS (1.36 vs. 2.07 years, HR 0.62 (0.50-0.77)), OS (4.84 vs. 5.81 years, HR 0.78 (0.61-0.99)) and DOR (1.48 vs. 2.08 years, HR 0.67 (0.53-0.86)). Furthermore, Rituximab improved survival across different MCL risk groups. In a post-hoc analysis of OS after relapse comparing patients receiving chemotherapy with / without rituximab, rituximab maintained efficacy with a median OS of 3.10 vs. 2.11 years (HR 0.70, 0.54-0.91). The rate of secondary malignancies was 0.5 and 3.9% for hematological and 7 and 8% for non-hematological malignancies for CHOP and R-CHOP patients, respectively. We present mature results of a pooled MCL cohort, demonstrating prolonged FFS, OS and DOR for the combined immuno-chemotherapy, confirming the standard of care in first line treatment.
Keywords: Immuno-chemotherapy; Long-term outcome; Mantle cell lymphoma; Rituximab.
© 2023. The Author(s).
Conflict of interest statement
Bittenbring JT received travel support and honoraria from Gilead, Incyte and MDS.
Hübel K served as an advisor and consultant for Roche, Celgene/BMS, Gilead, Incyte, EUSA, Novartis, received honoraria from Roche, Celgene/BMS, Servier, EUSA, BeiGene, Novartis and research support from Roche, Alexion, Celgene/BMS, Janssen, Incyte.
Schmidt C served as a consultant for Novartis, Kite/Gilead, Takeda, BMS, received honoraria from Novartis, Kite/Gilead, travel support from Novartis, Kite/Gilead, Takeda, BMS, Janssen and research funding from Kite/Gilead.
Glaß B served as a consultant for BMS, Roche, Riemser, Kite, Novartis, served in the speakers bureau of Roche and received research funding from Roche and Riemser.
Hüttmann A received honoraria from Celgene, Gilead, Takeda, served as a consultant for Lead Discovery Center GmbH and is a member of a Board or Advisory Committee for Takeda.
Hiddemann W received research support from Roche.
Unterhalt M received research support from Roche.
Dreyling M received speaker’s honoraria from Amgen, Astra Zeneca, Bayer, BMS/Celgene, Gilead/Kite, Incyte, Janssen, Novartis, Roche, served on scientific advisory bords for Astra Zeneca, Bayer, Beigene, BMS/Celgene, Genmab, Gilead/Kite, Incyte, Janssen, Lilly/Loxo, Morphosys, Novartis, Roche and received research support from Abbvie, Bayer, BMS/Celgene, Gilead/Kite, Janssen, Roche.
All remaining authors have declared no conflicts of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
