

Distribution and clinical impact of molecular subtypes with dark zone signature of DLBCL in a Japanese real-world study
- PMID: 37552496
- PMCID: PMC10758740
- DOI: 10.1182/bloodadvances.2023010402
Distribution and clinical impact of molecular subtypes with dark zone signature of DLBCL in a Japanese real-world study
Abstract
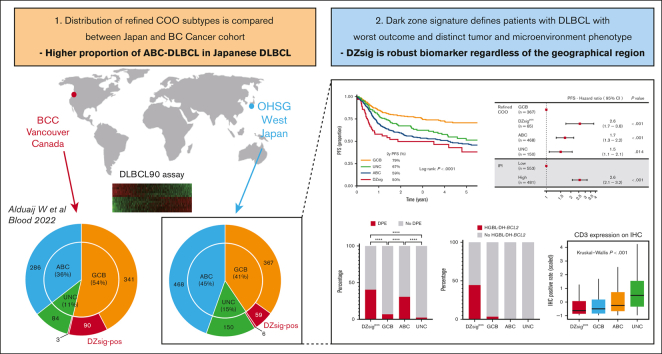
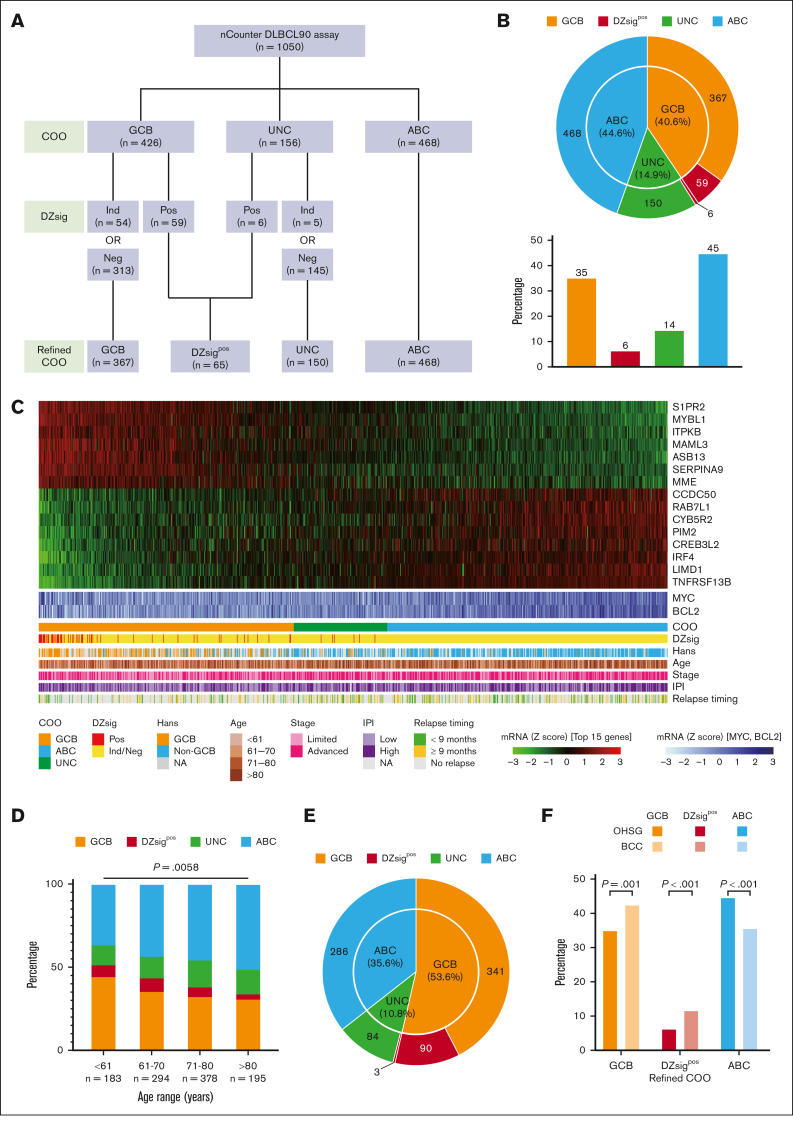
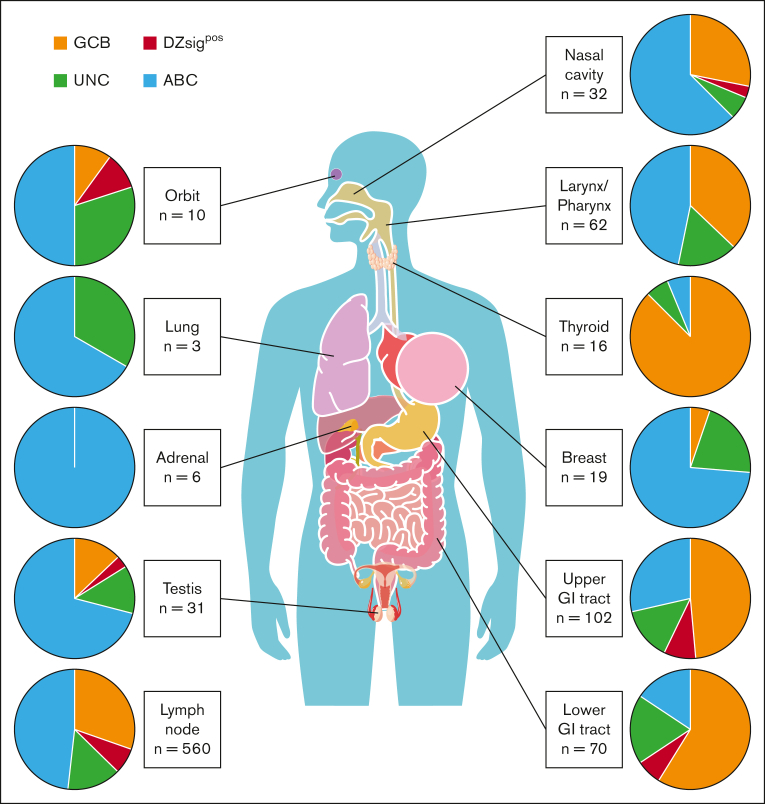
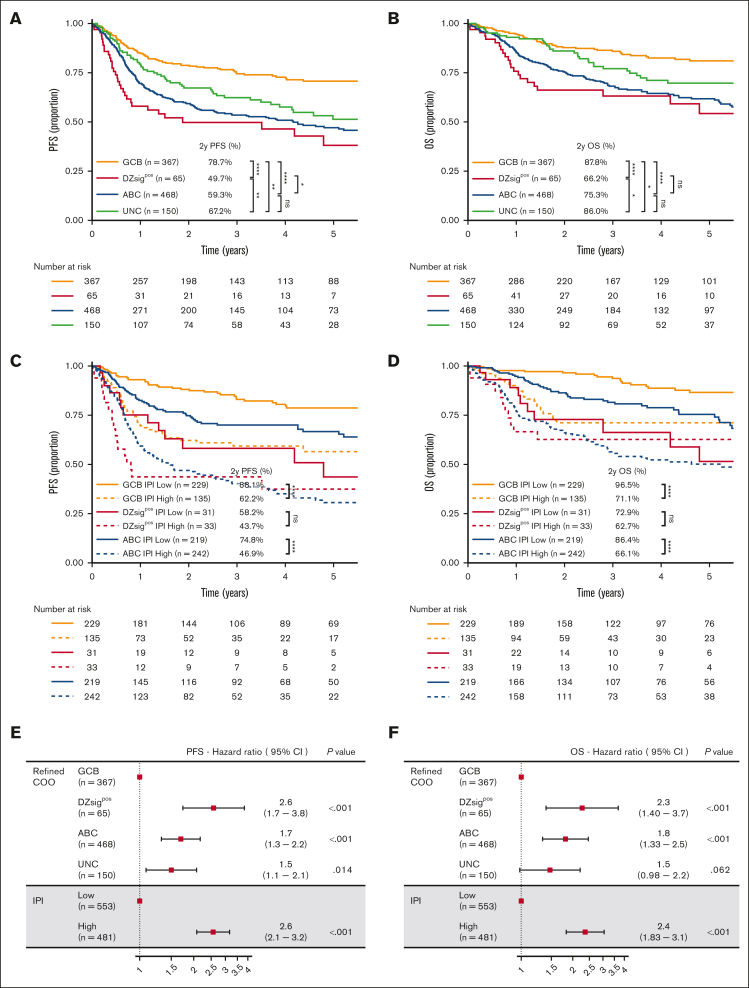
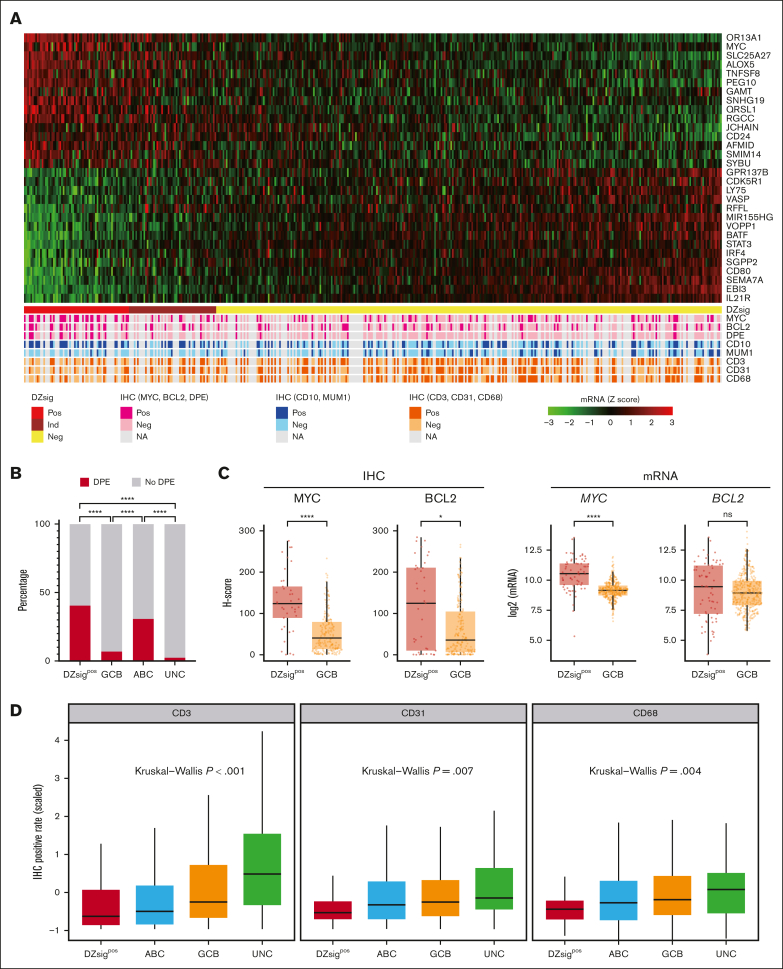
The distribution and clinical impact of cell-of-origin (COO) subtypes of diffuse large B-cell lymphoma (DLBCL) outside Western countries remain unknown. Recent literature also suggests that there is an additional COO subtype associated with the germinal center dark zone (DZ) that warrants wider validation to generalize clinical relevance. Here, we assembled a cohort of Japanese patients with untreated DLBCL and determined the refined COO subtypes, which include the DZ signature (DZsig), using the NanoString DLBCL90 assay. To compare the distribution and clinical characteristics of the molecular subtypes, we used a data set from the cohort of British Columbia Cancer (BCC) (n = 804). Through the 1050 patient samples on which DLBCL90 assay was successfully performed in our cohort, 35%, 45%, and 6% of patients were identified to have germinal center B-cell-like (GCB) DLBCL, activated B-cell-like (ABC) DLBCL, and DZsig-positive (DZsigpos) DLBCL, respectively, with the highest prevalence of ABC-DLBCL, differing significantly from the BCC result (P < .001). GCB-DLBCL, ABC-DLBCL, and DZsigpos-DLBCL were associated with 2-year overall survival rates of 88%, 75%, and 66%, respectively (P < .0001), with patients with DZsigpos-DLBCL having the poorest prognosis. In contrast, GCB-DLBCL without DZsig showed excellent outcomes after rituximab-containing immunochemotherapy. DZsigpos-DLBCL was associated with the significant enrichment of tumors with CD10 expression, concurrent MYC/BCL2 expression, and depletion of microenvironmental components (all, P < .05). These results provide evidence of the distinct distribution of clinically relevant molecular subtypes in Japanese DLBCL and that refined COO, as measured by the DLBCL90 assay, is a robust prognostic biomarker that is consistent across geographical areas.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: K. Sunami declares research funding and honoraria from Celgene, Sanofi, Bristol Myers Squibb (BMS), Ono, and Janssen, and research funding from Takeda, AbbVie, GlaxoSmithKline, Chugai, Otsuka, Merck Sharp and Dohme, Novartis, Astellas Amgen, Pfizer, Parexel, Kyowa Kirin, Symbio, and Agios. I.Y. declares research funding and honoraria from Kyowa Kirin and Chugai, and honoraria from Eisai, Janssen, Nippon-Shinyaku, Otsuka, Symbio, Takeda, Sumitomo Pharma, and Meiji. N.A. received honoraria from AbbVie. N.F. received honoraria from Novartis, Daiichi Sankyo, Chugai, Astellas, Janssen, and BMS. J.-i.T. declares research funding, honoraria, and speakers’ bureau fees from Takeda; honoraria and speakers, bureau fees from Chugai and BMS; and research funding from Nichirei and Ridgelinez. Y.M. declares research funding and scholarship donations from Chugai; research funding from Nippon Shinyaku; and scholarship donations from Eisai, Otsuka, Kyowa Kirin, and Takeda. D.W.S. declares consultancy for AbbVie and Incyte; consultancy for and honoraria from AstraZeneca; consultancy for and research funding from Janssen; research funding from Roche; and patent with NanoString. D.E. declares research funding from Nippon Shinyaku; honoraria from Eisai and Kyowa Kirin; and research funding and honoraria from Chugai. The remaining authors declare no competing financial interests.
Figures
References
-
- Alizadeh AA, Eisen MB, Davis RE, et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403(6769):503–511. - PubMed
-
- Shipp MA, Ross KN, Tamayo P, et al. Diffuse large B-cell lymphoma outcome prediction by gene-expression profiling and supervised machine learning. Nat Med. 2002;8(1):68–74. - PubMed
-
- Hans CP, Weisenburger DD, Greiner TC, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103(1):275–282. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
