

Conservative versus Liberal Oxygenation Targets in Intensive Care Unit Patients (ICONIC): A Randomized Clinical Trial
- PMID: 37552556
- PMCID: PMC10563190
- DOI: 10.1164/rccm.202303-0560OC
Conservative versus Liberal Oxygenation Targets in Intensive Care Unit Patients (ICONIC): A Randomized Clinical Trial
Abstract
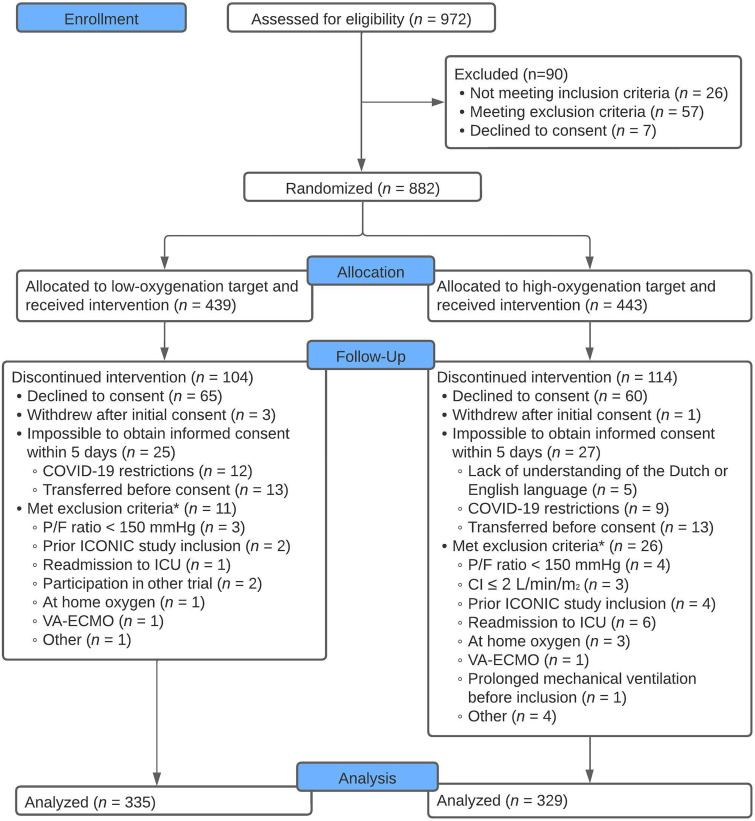
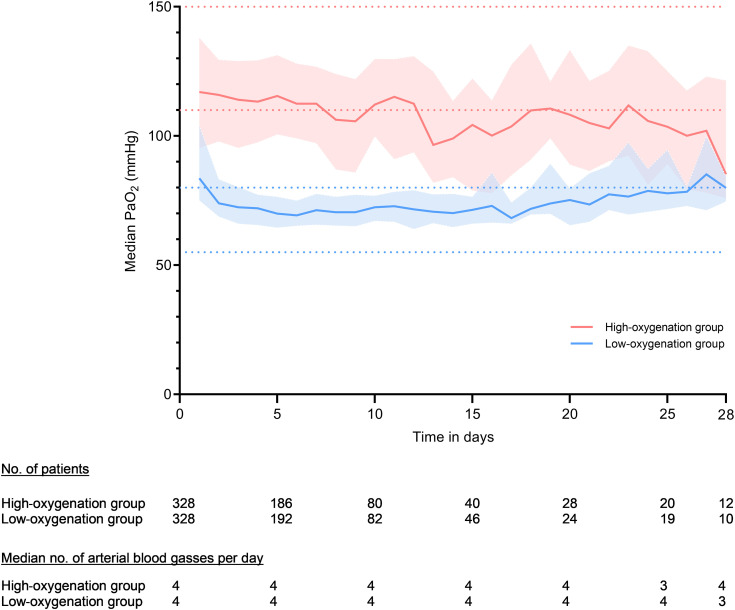
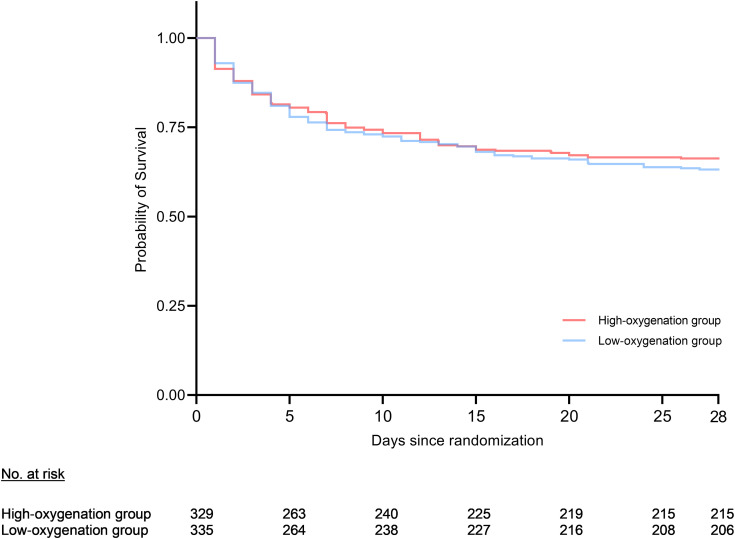
Rationale: Supplemental oxygen is widely administered to ICU patients, but appropriate oxygenation targets remain unclear. Objectives: This study aimed to determine whether a low-oxygenation strategy would lower 28-day mortality compared with a high-oxygenation strategy. Methods: This randomized multicenter trial included mechanically ventilated ICU patients with an expected ventilation duration of at least 24 hours. Patients were randomized 1:1 to a low-oxygenation (PaO2, 55-80 mm Hg; or oxygen saturation as measured by pulse oximetry, 91-94%) or high-oxygenation (PaO2, 110-150 mm Hg; or oxygen saturation as measured by pulse oximetry, 96-100%) target until ICU discharge or 28 days after randomization, whichever came first. The primary outcome was 28-day mortality. The study was stopped prematurely because of the COVID-19 pandemic when 664 of the planned 1,512 patients were included. Measurements and Main Results: Between November 2018 and November 2021, a total of 664 patients were included in the trial: 335 in the low-oxygenation group and 329 in the high-oxygenation group. The median achieved PaO2 was 75 mm Hg (interquartile range, 70-84) and 115 mm Hg (interquartile range, 100-129) in the low- and high-oxygenation groups, respectively. At Day 28, 129 (38.5%) and 114 (34.7%) patients had died in the low- and high-oxygenation groups, respectively (risk ratio, 1.11; 95% confidence interval, 0.9-1.4; P = 0.30). At least one serious adverse event was reported in 12 (3.6%) and 17 (5.2%) patients in the low- and high-oxygenation groups, respectively. Conclusions: Among mechanically ventilated ICU patients with an expected mechanical ventilation duration of at least 24 hours, using a low-oxygenation strategy did not result in a reduction of 28-day mortality compared with a high-oxygenation strategy. Clinical trial registered with the National Trial Register and the International Clinical Trials Registry Platform (NTR7376).
Keywords: hyperoxia; hypoxia; intensive care medicine; mechanical ventilation; oxygen.
Figures
Comment in
-
Oxygen Targets and the Future of Critical Care Clinical Research.Am J Respir Crit Care Med. 2023 Oct 1;208(7):746-748. doi: 10.1164/rccm.202308-1417ED. Am J Respir Crit Care Med. 2023. PMID: 37610828 Free PMC article. No abstract available.
References
-
- Knighton DR, Halliday B, Hunt TK. Oxygen as an antibiotic. The effect of inspired oxygen on infection. Arch Surg . 1984;119:199–204. - PubMed
-
- Helmerhorst HJ, Arts DL, Schultz MJ, van der Voort PH, Abu-Hanna A, de Jonge E, et al. Metrics of arterial hyperoxia and associated outcomes in critical care. Crit Care Med . 2017;45:187–195. - PubMed
-
- Helmerhorst HJ, Roos-Blom MJ, van Westerloo DJ, de Jonge E. Association between arterial hyperoxia and outcome in subsets of critical illness: a systematic review, meta-analysis, and meta-regression of cohort studies. Crit Care Med . 2015;43:1508–1519. - PubMed
-
- Asfar P, Singer M, Radermacher P. Understanding the benefits and harms of oxygen therapy. Intensive Care Med . 2015;41:1118–1121. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
