

Improved patient-reported outcomes after open preperitoneal inguinal hernia repair compared to anterior Lichtenstein repair: 10-year ACHQC analysis
- PMID: 37553502
- PMCID: PMC10533599
- DOI: 10.1007/s10029-023-02852-6
Improved patient-reported outcomes after open preperitoneal inguinal hernia repair compared to anterior Lichtenstein repair: 10-year ACHQC analysis
Abstract
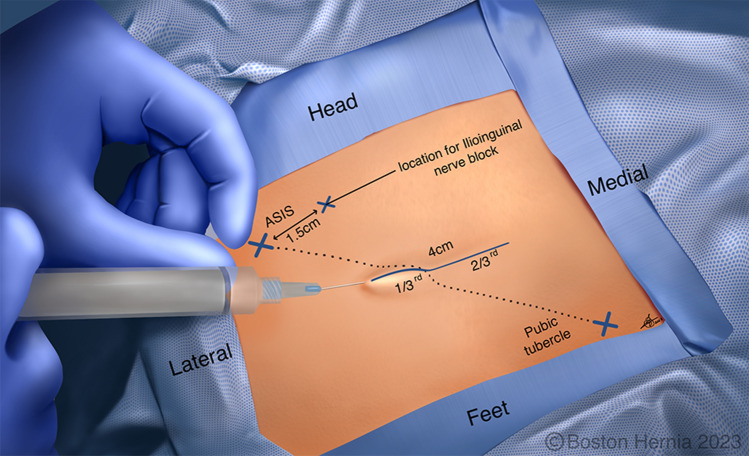
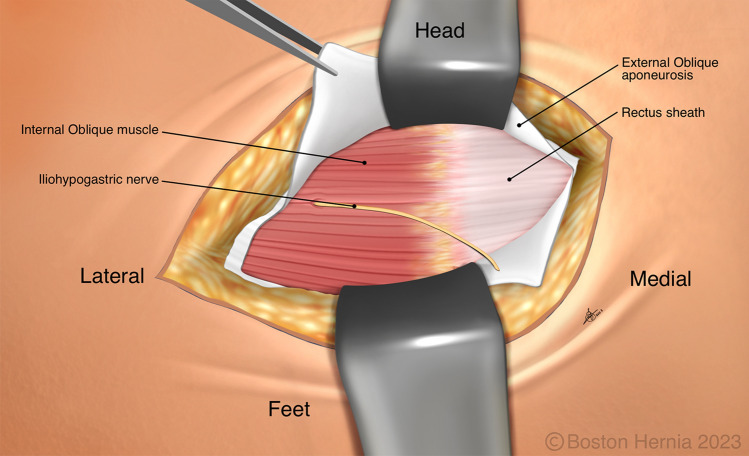
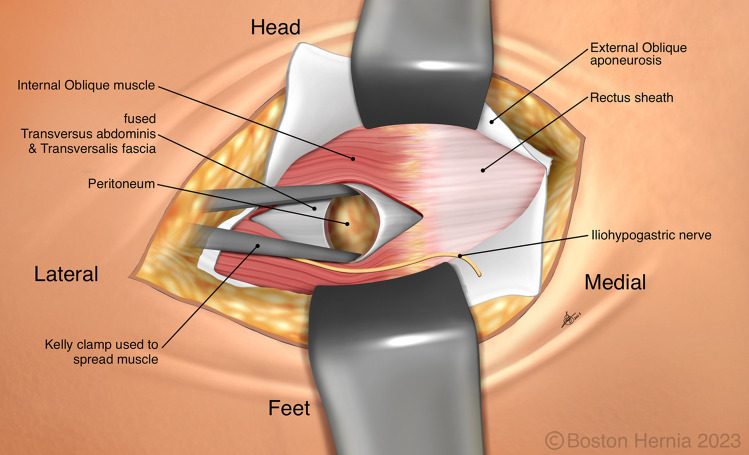
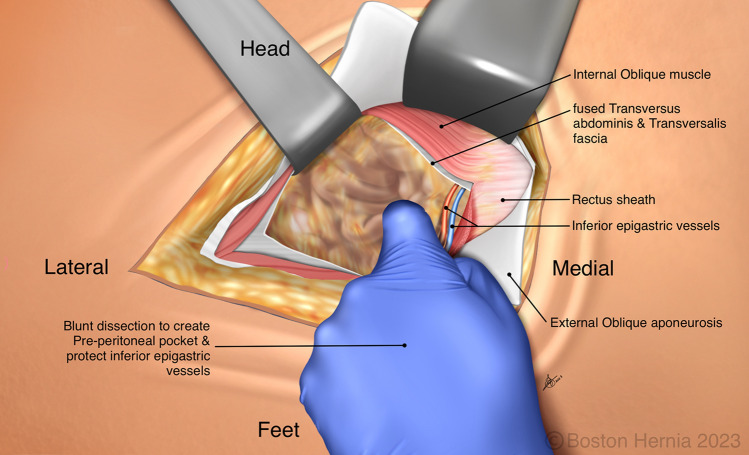
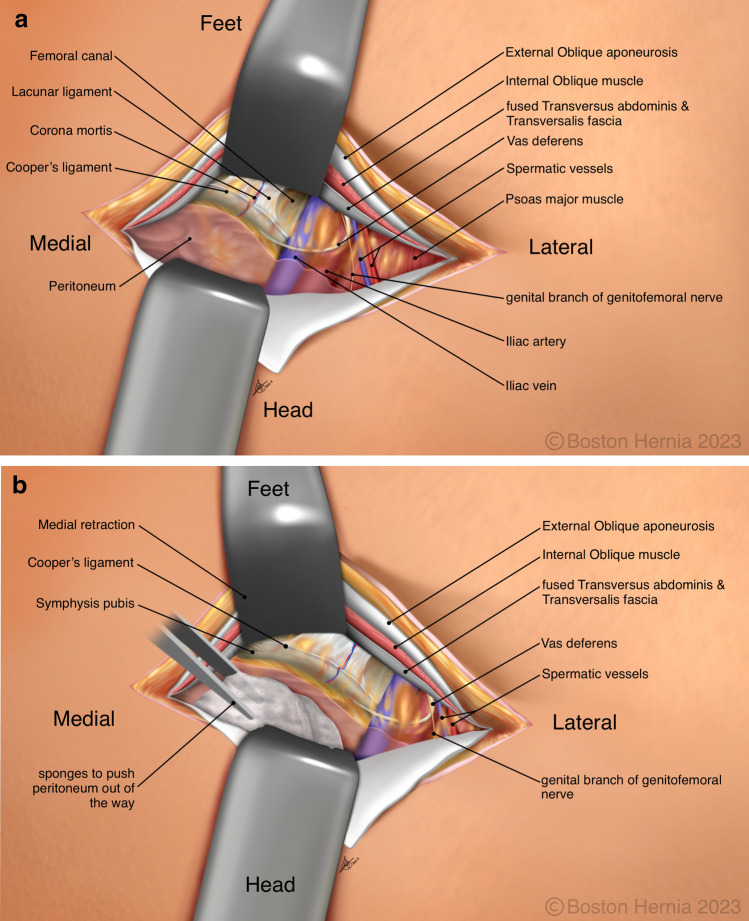
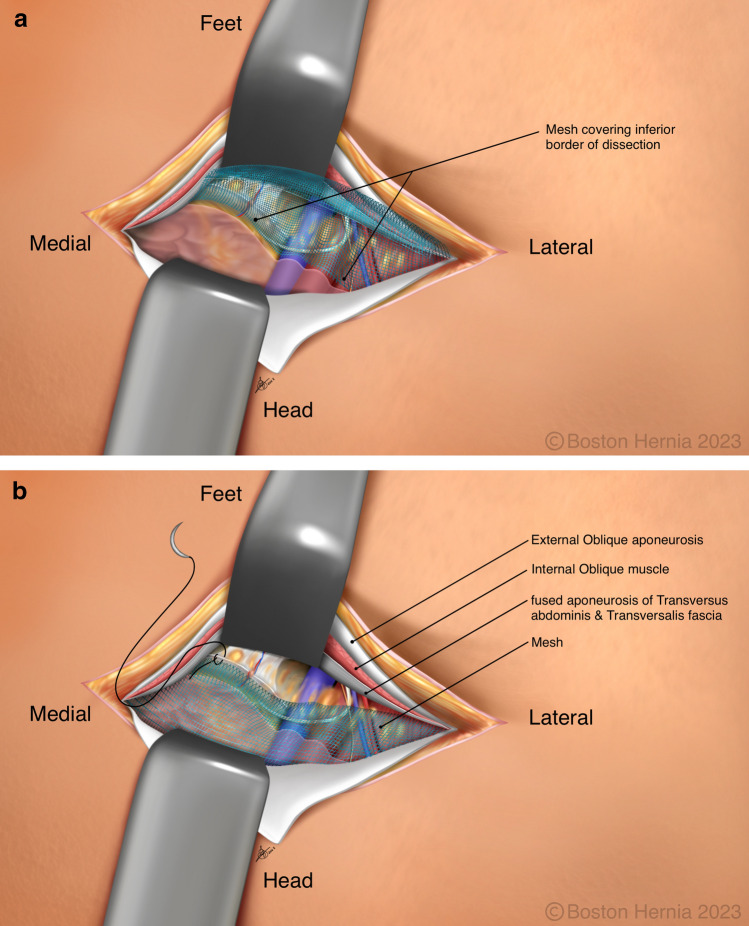
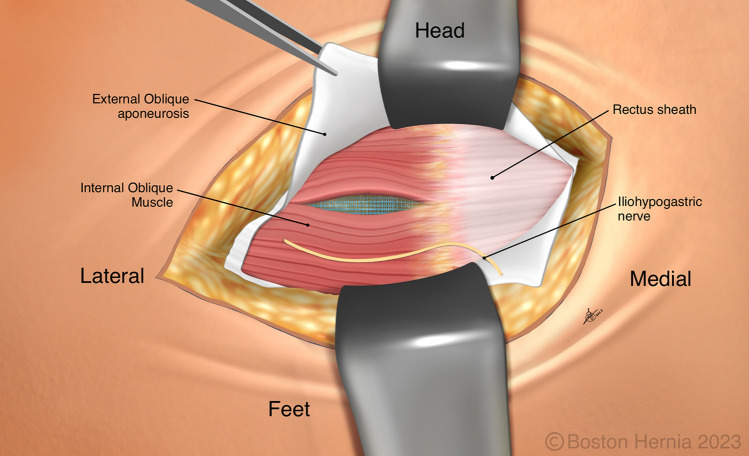
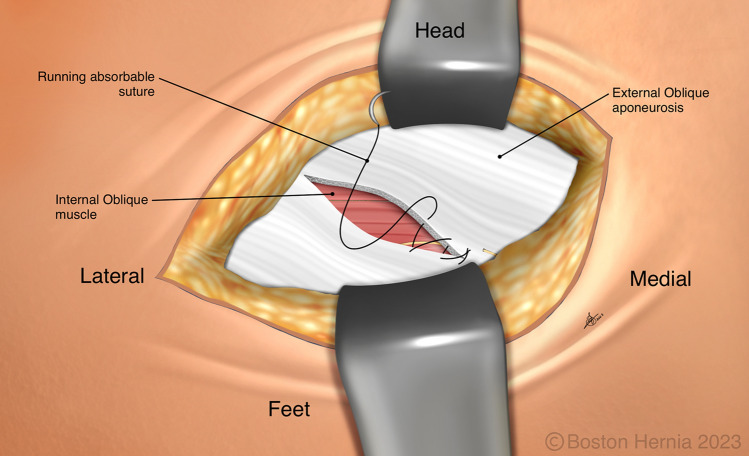
Introduction: The Lichtenstein repair has been synonymous with "open" inguinal hernia repair (IHR) for 40 years. However, international guidelines have suggested that posterior mesh placement results in advantageous biomechanics and reduced risk of nerve-related chronic pain. Additionally, the use of local anesthetics has been shown to reduce postoperative pain and complication risks. An open transrectus preperitoneal/open preperitoneal (TREPP/OPP) repair combines posterior mesh placement with the use of local anesthetic and as such could be the ideal repair for primary inguinal hernia. Using the Abdominal Core Health Quality Collaborative (ACHQC) registry, we compared open anterior mesh with open posterior mesh repairs.
Methods: We performed a propensity score matched analysis of patients undergoing open IHR between 2012 and 2022 in the ACHQC. After 1:1 optimal matching, both the TREPP/OPP and Lichtenstein cohorts were balanced with 451 participants in each group. Outcomes included patient-reported quality of life (QoL), hernia recurrence, and postoperative opioid use.
Results: Improvement was seen after TREPP/OPP in EuraHS QoL score at 30 days (OR 0.558 [0.408, 0.761]; p = 0.001), and the difference persisted at 1 year (OR 0.588 [0.346, 0.994]; p = 0.047). Patient-reported opioid use at 30-day follow-up was significantly lower in the TREPP/OPP cohort (OR 0.31 [0.20, 0.48]; p < 0.001). 30-day frequency of surgical-site occurrences was significantly higher in the Lichtenstein repair cohort (OR 0.22 [0.06-0.61]; p = 0.007). There were no statistically significant differences in hernia recurrence risk at 1 year, or rates of postoperative bleeding, peripheral nerve injury, DVTs, or UTIs.
Conclusion: Our analysis demonstrates a benefit of posterior mesh placement (TREPP/OPP) over anterior mesh placement (Lichtenstein) in open inguinal hernia repair in patient-reported QoL and reduced opioid use.
Keywords: Inguinal hernia; Lichtenstein; Preperitoneal repair; Quality-of-life; TREPP/OPP.
© 2023. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures


Comment in
-
Delivering what inguinal hernia patients really really want.Hernia. 2023 Dec;27(6):1617. doi: 10.1007/s10029-023-02899-5. Epub 2023 Oct 30. Hernia. 2023. PMID: 37902890 No abstract available.
References
-
- Hassler KR, Saxena P, Baltazar-Ford KS. StatPearls. Treasure Island (FL): StatPearls Publishing; 2022. Open inguinal hernia repair. - PubMed
-
- Komorowski AL. History of the inguinal hernia repair. IntechOpen; 2014.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
