

Clinical outcomes of parenchymal-sparing versus anatomic resection for colorectal liver metastases: a systematic review and meta-analysis
- PMID: 37553574
- PMCID: PMC10408219
- DOI: 10.1186/s12957-023-03127-1
Clinical outcomes of parenchymal-sparing versus anatomic resection for colorectal liver metastases: a systematic review and meta-analysis
Abstract
Background: The advantages of parenchymal-sparing resection (PSR) over anatomic resection (AR) of colorectal liver metastases (CRLM) remain controversial. Here, we aim to evaluate their safety and efficacy.
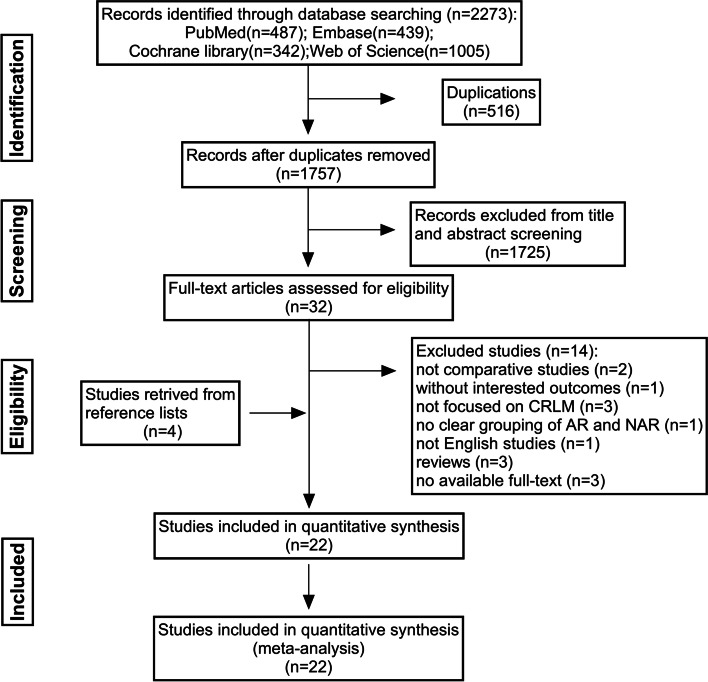
Methods: A systematic review and meta-analysis of short-term perioperative outcomes and long-term oncological outcomes for PSR and AR were performed by searching Pubmed, Embase, the Cochrane Library and Web of Science databases.
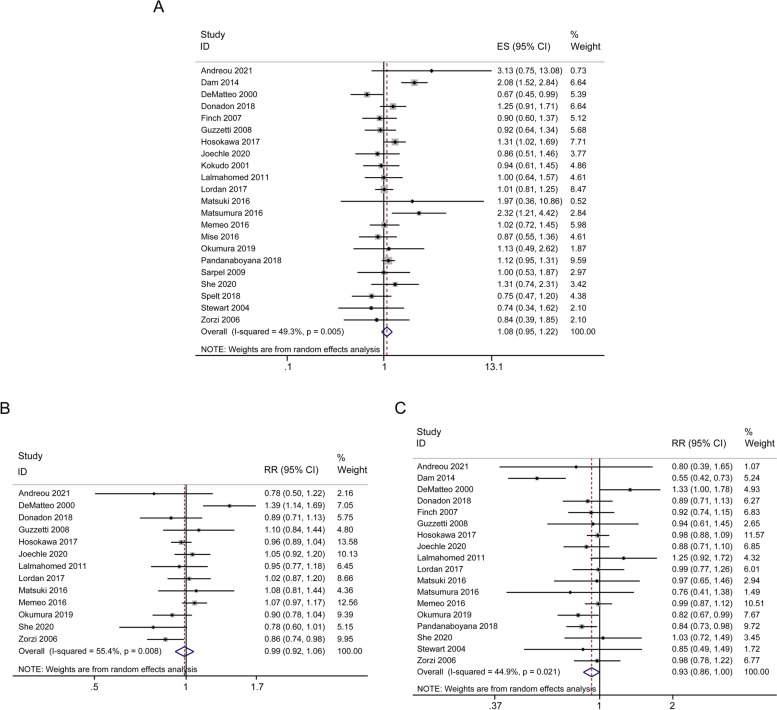
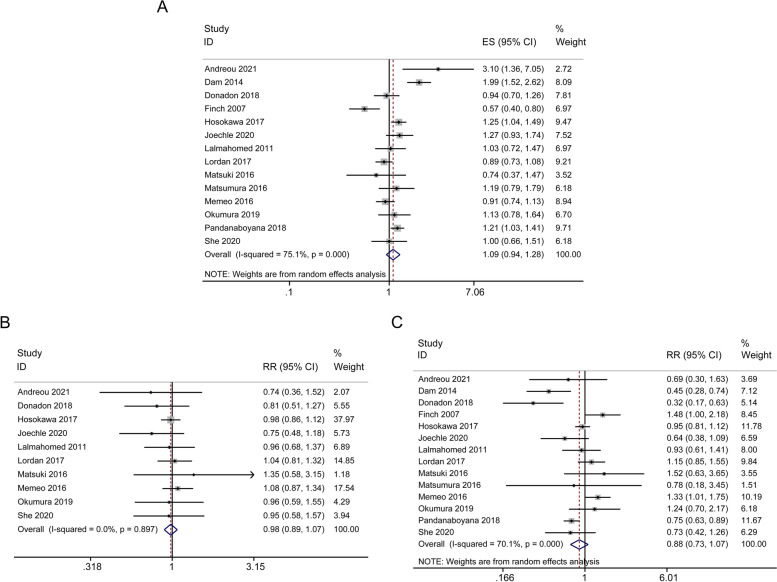
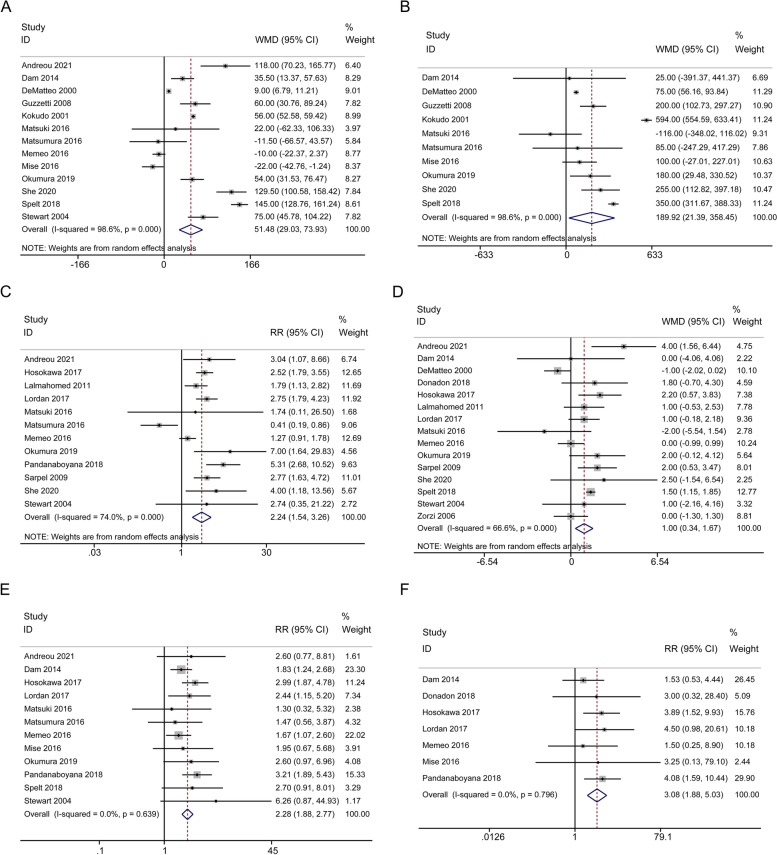
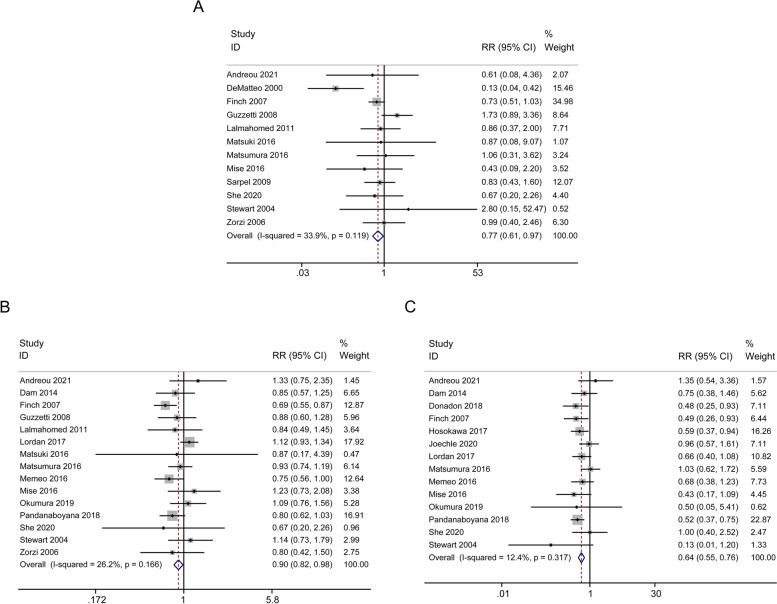
Results: Twenty-two studies were considered eligible (totally 7228 patients: AR, n = 3154 (43.6%) vs. PSR, n = 4074 (56.4%)). Overall survival (OS, HR = 1.08, 95% CI: 0.95-1.22, P = 0.245) and disease-free survival (DFS, HR = 1.09, 95% CI: 0.94-1.28, P = 0.259) were comparable between the two groups. There were no significant differences in 3-year OS, 5-year OS, 3-year DFS, 5-year DFS, 3-year liver recurrence-free survival (liver-RFS) and 5-year liver-RFS. In terms of perioperative outcome, patients undergoing AR surgery were associated with prolonged operation time (WMD = 51.48 min, 95% CI: 29.03-73.93, P < 0.001), higher amount of blood loss (WMD = 189.92 ml, 95% CI: 21.39-358.45, P = 0.027), increased intraoperative blood transfusion rate (RR = 2.24, 95% CI: 1.54-3.26, P < 0.001), prolonged hospital stay (WMD = 1.00 day, 95% CI: 0.34-1.67, P = 0.003), postoperative complications (RR = 2.28, 95% CI: 1.88-2.77, P < 0.001), and 90-day mortality (RR = 3.08, 95% CI: 1.88-5.03, P < 0.001). While PSR surgery was associated with positive resection margins (RR = 0.77, 95% CI: 0.61-0.97, P = 0.024), intrahepatic recurrence (RR = 0.90, 95% CI: 0.82-0.98, P = 0.021) and repeat hepatectomy (RR = 0.64, 95% CI: 0.55-0.76, P < 0.001).
Conclusion: Considering relatively acceptable heterogeneity, PSR had better perioperative outcomes without compromising oncological long-term outcomes. However, these findings must be carefully interpreted, requiring more supporting evidence.
Trial registration: PROSPERO registration number: CRD42023445332.
Keywords: Anatomic resection; Colorectal liver metastases; Meta-analysis; Outcomes; Parenchymal-sparing resection.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233–254. - PubMed
-
- Ciardiello F, Ciardiello D, Martini G, Napolitano S, Tabernero J, Cervantes A. Clinical management of metastatic colorectal cancer in the era of precision medicine. CA Cancer J Clin. 2022;72(4):372–401. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
