

Maintenance lenalidomide in newly diagnosed transplant eligible and non-eligible myeloma patients; profiling second primary malignancies in 4358 patients treated in the Myeloma XI Trial
- PMID: 37554123
- PMCID: PMC10404862
- DOI: 10.1016/j.eclinm.2023.102099
Maintenance lenalidomide in newly diagnosed transplant eligible and non-eligible myeloma patients; profiling second primary malignancies in 4358 patients treated in the Myeloma XI Trial
Abstract
Background: Early trials of long-term lenalidomide use reported an increased incidence of second primary malignancy (SPM), including acute myeloid leukaemia and myelodysplastic syndrome. Later, meta-analysis suggested the link to be secondary to lenalidomide in combination with melphalan.
Methods: Myeloma XI is a large, phase III randomised trial in-which lenalidomide was used at induction and maintenance, in transplant eligible (TE) and non-eligible (TNE) newly diagnosed patients (NCT01554852). Here we present an analysis of SPM incidence and profile the SPM type to determine the impact of autologous stem cell transplantation (ASCT) and lenalidomide exposure in 4358 patients treated on study. Data collection took place from the start of the trial in May 2010, to May 2019, as per the protocol timeline. The Median follow-up following maintenance randomisation was 54.5 and 46.1 months for TE and TNE patients, respectively.
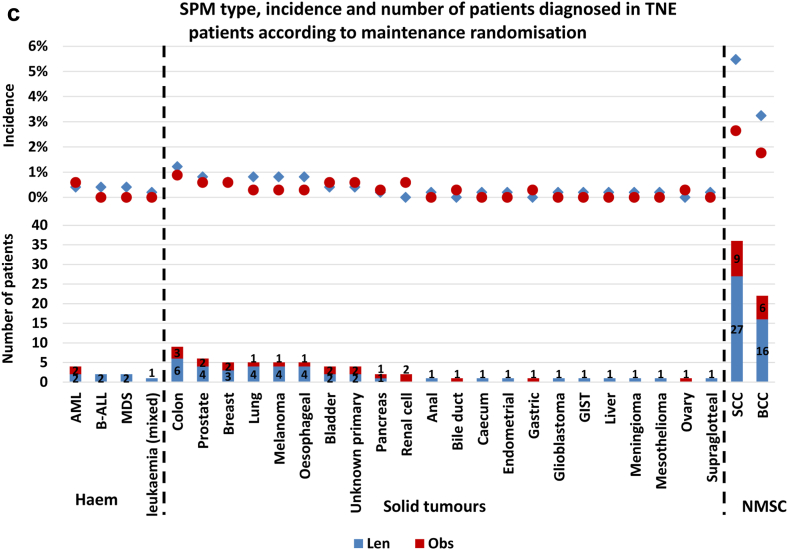
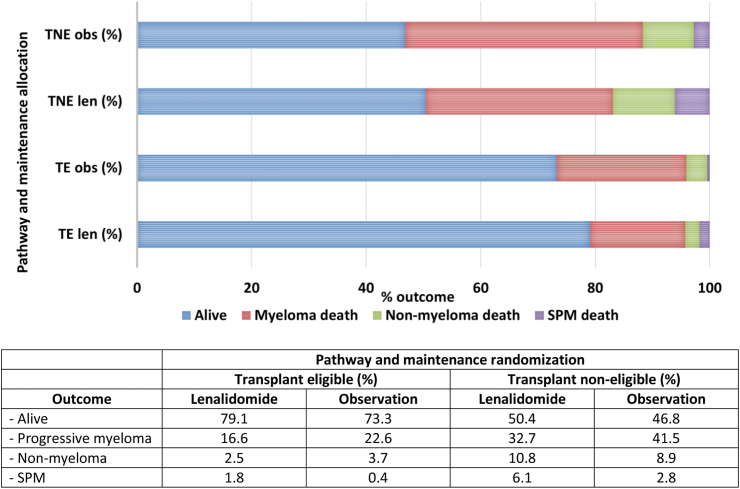
Findings: In the TE pathway, the overall SPM incidence was 7.7% in lenalidomide maintenance patients compared to 3.2% in those being observed (p = 0.006). Although the TNE lenalidomide maintenance patients had the greatest SPM incidence (15.4%), this was not statistically significant when compared to the observed patients (10%, p = 0.10).The SPM incidence was higher in patients who received lenalidomide at induction and maintenance (double exposure), when compared to those treated with lenalidomide at one time point (single exposure). Again, this was most marked in TNE patients where the overall SPM incidence was 16.9% in double exposed patients, compared to 11.7% in single exposed patients, and 11.2% in patients who did not receive lenalidomide (p = 0.04). This is likely an effect of treatment duration, with the median number of cycles being 27 in the TNE double exposed patients, vs 6 in the single exposure patients.Haematological SPMs were uncommon, diagnosed in 50 patients (incidence 1.1%). The majority of cases were diagnosed in TE patients treated with lenalidomide maintenance (n = 25, incidence 2.8%), suggesting a possible link with melphalan. Non-melanoma skin cancer incidence was highest in patients receiving lenalidomide maintenance, particularly in TNE patients, where squamous cell carcinoma and basal cell carcinoma were diagnosed in 5.5% and 2.6% of patients, respectively. The incidence of most solid tumour types was higher in lenalidomide maintenance patients.Mortality due to progressive myeloma was reduced in patients receiving lenalidomide maintenance, noted to be 16.6% compared 22.6% in those observed in TE patients and 32.7% compared to 41.5% in TNE patients. SPM related mortality was low, 1.8% and 6.1% in TE and TNE lenalidomide maintenance patients, respectively, compared to 0.4% and 2.8% in those being observed.
Interpretation: This provides reassurance that long-term lenalidomide treatment is safe and associated with improved outcomes in TE and TNE populations, although monitoring for SPM development should be incorporated into clinic review processes.
Funding: Primary financial support was from Cancer Research UK [C1298/A10410].
Keywords: Lenalidomide; Lenalidomide maintenance; Myeloma; SPM; Second primary malignancy; Transplant eligible; Transplant non-eligible.
© 2023 The Authors.
Conflict of interest statement
DAC is a DSMB statistician for academically led investigator-initiated study in multiple myeloma; CP has received honoraria, undertaken consultancy and received research funding from BMS/Celgene; AB has received honoraria from BMS/Celgene, GSK, Sanofi, Amgen, Takeda and Janssen, received travel support from Amgen, Sanofi and BMS/Celgene, and undertaken consultancy for BMS/Celgene, Janssen, Takeda and Sanofi. MWJ has received honoraria from Pfizer, Janssen, BMS and Sanofi, and received meeting support from Janssen and Merinari Stemline; MFK has received research funding from BMS/Celgene and Janssen, honoraria from BMS/Celgene, Takeda and Abbvie and undertaken consultancy for Adaptive, Abbvie, BMS/Celgene, Pfizer, GSK, Karyopharm and Seattle Genetics; RGO has undertaken consultancy from Janssen and Beigene, received honoraria from Astra Zeneca, Janssen and Beigene, and received meeting support from Beigene; GHJ has received honoraria and research funding from BMS/Celgene. Celgene corporation, Merck Sharpe and Dohme and Amgen have provided unrestricted educational grants relating to this study, paid to the Clinical Trials Research Unit, University of Leeds.
Figures





References
-
- Attal M., Lauwers-Cances V., Marit G., et al. Lenalidomide maintenance after stem-cell transplantation for multiple myeloma. N Engl J Med. 2012;366(19):1782–1791. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
