

Toxicity profile of antibody-drug conjugates in breast cancer: practical considerations
- PMID: 37554126
- PMCID: PMC10404866
- DOI: 10.1016/j.eclinm.2023.102113
Toxicity profile of antibody-drug conjugates in breast cancer: practical considerations
Abstract
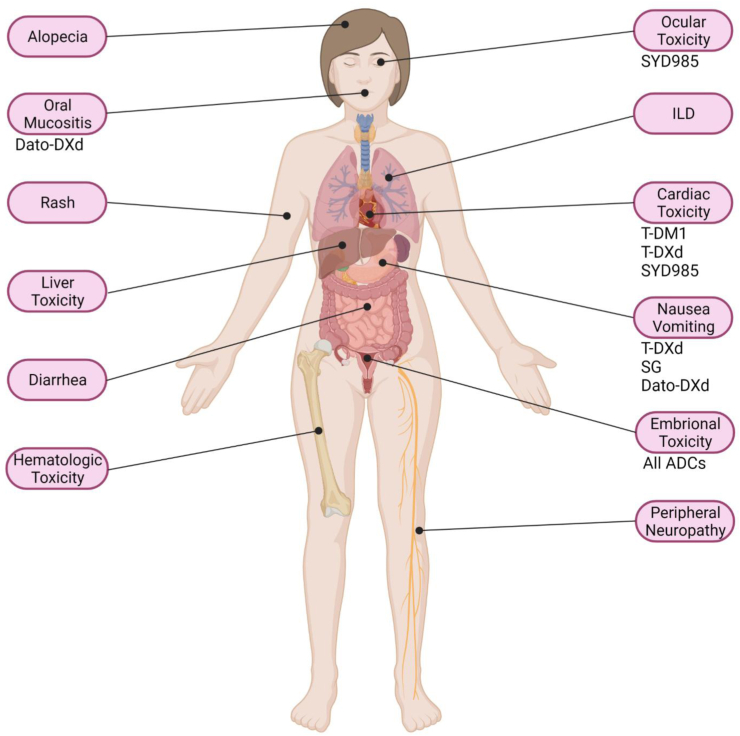
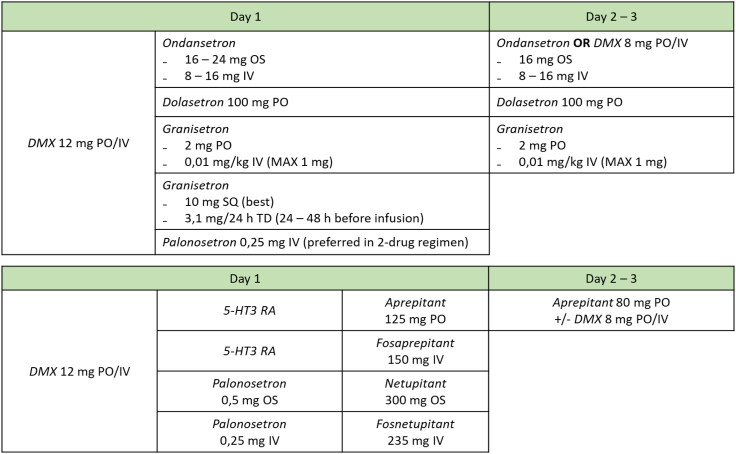
Antibody-drug conjugates (ADCs) represent a novel and evolving class of antineoplastic agents, constituted by monoclonal antibody linked to biologically active drugs, delivering cytotoxic compounds at the tumor site, reducing the likelihood of systemic exposure and toxicity. They are generally well tolerated, nevertheless some predictable adverse reactions need careful monitoring and timely approach. These include neutropenia, nausea and vomiting, alopecia, diarrhea, left ventricular dysfunction, ILD/pneumonitis. The mechanisms leading to drug-associated toxicities are summarized, and prophylaxis protocols and appropriate management strategies are proposed, based on current literature. This review aims to collect the most updated evidence on toxicities potentially occurring during breast cancer treatment with approved or under clinical investigation (advanced stage) ADCs. A focus is dedicated to monitoring protocols and clinical management, aimed at preventing and/or promptly address relevant problems, in order to avoid premature discontinuation or improper dose reduction.
Keywords: Antibody drug conjugates; Breast cancer; Toxicity management.
© 2023 The Author(s).
Conflict of interest statement
AV has received travel grants from Lilly, Novartis, Pierre Fabre, and Gilead. MP has received travel grants from Pfizer and Gilead. RC declares honoraria from Novartis, Lilly, Gilead, Seagen, Veracyte, Daichii Sankyo, Pierre-Fabre; she is advisory board member for Novartis, Lilly, Gilead, Seagen, Daichii Sankyo, Pierre-Fabre, Roche, Astra Zeneca, and MSD; she has received travel grants from Gilead, Lilly and Novartis. FP received honoraria for advisory boards, activities as a speaker, travel grants, research grants from AstraZeneca, Daichii Sankyo, Eisai, Lilly, Gilead, MSD, Novartis, Exact Sciences, Menarini, Pierre Fabre, Pfizer, Roche, and Seagen. He has received research funding from AstraZeneca, Eisai and Roche. MG is a consultant/advisory board member for AstraZeneca, Daichii Sankyo, Eisai, Gilead, Lilly, MSD, Novartis, Pfizer, and Seagen; he has received travel grants from AstraZeneca, Pfizer and research funding (to institution) from AstraZeneca. LDM is a consultant/advisory board member for Lilly, Novartis, Roche, Pfizer, Daiichi Sankyo, Exact science, Gilead, Pierre Fabre, Eisai, AstraZeneca, GSK, Seagen, and Agendia; she has received research support from Roche, Lilly, Seagen, Daiichi Sankyo and Novartis (to institution); she declares honoraria from Roche, Pfizer, Lilly, MSD, Seagen, Gilead, Pierre Fabre, Eisai, Ipsen, Exact science, AstraZeneca and Novartis; has received travel grants from Roche, Pfizer, Eisai, AstraZeneca, and Daiichi Sankyo. GA is a consultant/advisory board member for Roche, Lilly, AstraZeneca, Novartis, Seagen, Daiichi Sankyo, Eisai, and Gilead; she has received research support from AstraZeneca (to institution); declares honoraria from Roche, Pfizer, Lilly, Eisai, AstraZeneca, Gilead, Seagen, Viatris, Exact Sciences, Daiichi Sankyo, and Novartis; has received travel grants from Roche, Daiichi Sankyo, and Novartis. MDL is a consultant/advisory board member for Pfizer, AstraZeneca, Sanofi, Seagen, Novartis, Ipsen, Roche, Pierre Fabre, Daiichi Sankyo, and GSK; he declares honoraria from Lilly, Novartis, Seagen, Takeda, Roche, Daiichi Sankyo, Tomalab, Gilead, Genetic, Menarini, and Sophos; has received travel grants from Roche, AstraZeneca. FM is a consultant/advisory board member for Roche, Daiichi Sankyo, Seagen; he received honoraria from Roche, AstraZeneca, Daiichi Sankyo, Seagen Pierre Fabre, MSD, Novartis, and Pfizer; he has received travel grants from AstraZeneca. AD, FN, SP, and MV have no conflict of interest to declare.
Figures
References
-
- Sakach E., Sacks R., Kalinsky K. Trop-2 as a therapeutic target in breast cancer. Cancers. 2022;14:5936. https://www.mdpi.com/2072-6694/14/23/5936/htm [cited 2023 Mar 17]Available from: - PMC - PubMed
-
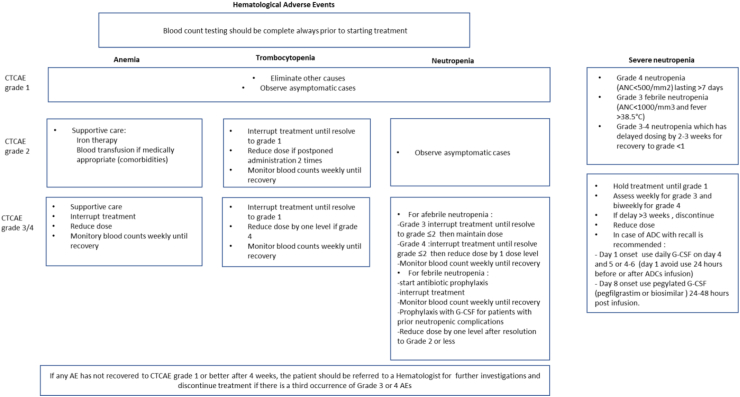
- U.S. Department of Health and Human Serivices, National Institutes of Health National Cancer Institute, Common Terminology Criteria for Adverse Events (CTCAE) V. 5.0. 2017
-
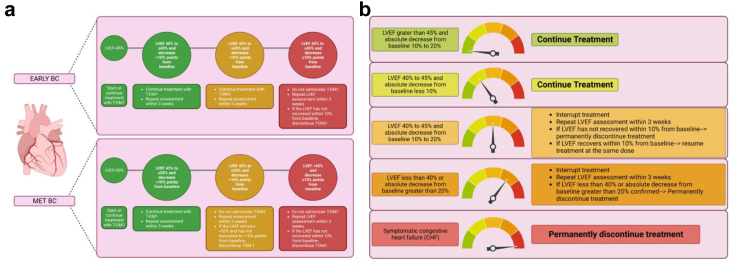
- Krop I.E., Kim S.-B.B., González-Martín A., et al. Trastuzumab emtansine versus treatment of physician’s choice for pretreated HER2-positive advanced breast cancer (TH3RESA): a randomised, open-label, phase 3 trial. Lancet Oncol. 2014;15(7):689–699. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
