

Cardiovascular responses to hot skin at rest and during exercise
- PMID: 37554384
- PMCID: PMC10405766
- DOI: 10.1080/23328940.2022.2109931
Cardiovascular responses to hot skin at rest and during exercise
Abstract
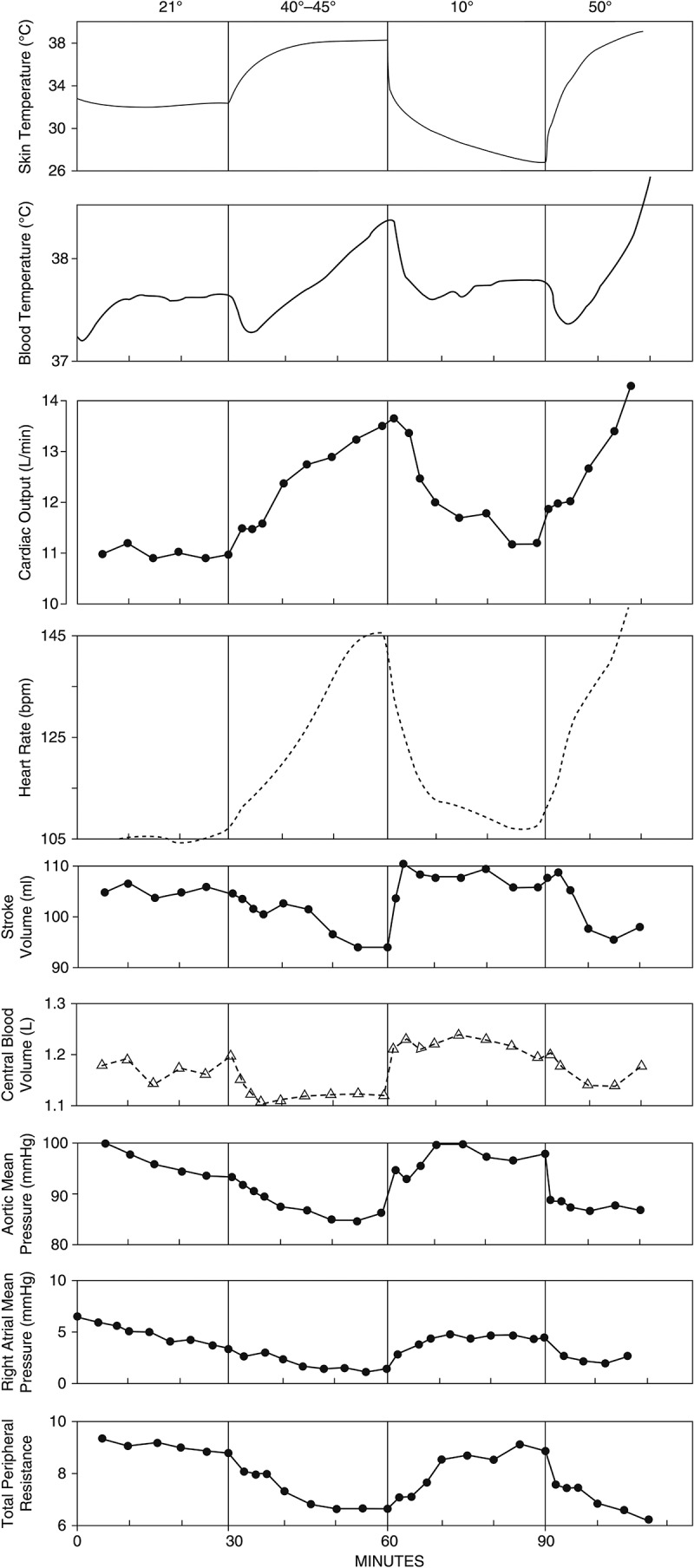
Integrative cardiovascular responses to heat stress during endurance exercise depend on various variables, such as thermal stress and exercise intensity. This review addresses how increases in skin temperature alter and challenge the integrative cardiovascular system during upright submaximal endurance exercise, especially when skin is hot (i.e. >38°C). Current evidence suggests that exercise intensity plays a significant role in cardiovascular responses to hot skin during exercise. At rest and during mild intensity exercise, hot skin increases skin blood flow and abolishes cutaneous venous tone, which causes blood pooling in the skin while having little impact on stroke volume and thus cardiac output is increased with an increase in heart rate. When the heart rate is at relatively low levels, small increases in heart rate, skin blood flow, and cutaneous venous volume do not compromise stroke volume, so cardiac output can increase to fulfill the demands for maintaining blood pressure, heat dissipation, and the exercising muscle. On the contrary, during more intense exercise, hot skin does not abolish exercise-induced cutaneous venoconstriction possibly due to high sympathetic nerve activities; thus, it does not cause blood pooling in the skin. However, hot skin reduces stroke volume, which is associated with a decrease in ventricular filling time caused by an increase in heart rate. When the heart rate is high during moderate or intense exercise, even a slight reduction in ventricular filling time lowers stroke volume. Cardiac output is therefore not elevated when skin is hot during moderate intensity exercise.
Keywords: Skin temperature; cardiovascular control; cutaneous venous volume; heat stress; hemodynamic; hyperthermia; skin blood flow.
© 2022 Informa UK Limited, trading as Taylor & Francis Group.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures











Similar articles
-
Cardiovascular responses to exercise when increasing skin temperature with narrowing of the core-to-skin temperature gradient.J Appl Physiol (1985). 2018 Sep 1;125(3):697-705. doi: 10.1152/japplphysiol.00965.2017. Epub 2018 May 10. J Appl Physiol (1985). 2018. PMID: 29745802
-
Low Stroke Volume during Exercise with Hot Skin Is Due to Elevated Heart Rate.Med Sci Sports Exerc. 2019 Oct;51(10):2025-2032. doi: 10.1249/MSS.0000000000002029. Med Sci Sports Exerc. 2019. PMID: 31058763
-
Cardiovascular strain impairs prolonged self-paced exercise in the heat.Exp Physiol. 2011 Feb;96(2):134-44. doi: 10.1113/expphysiol.2010.054213. Epub 2010 Sep 17. Exp Physiol. 2011. PMID: 20851861
-
Cardiovascular adaptations supporting human exercise-heat acclimation.Auton Neurosci. 2016 Apr;196:52-62. doi: 10.1016/j.autneu.2016.02.002. Epub 2016 Feb 12. Auton Neurosci. 2016. PMID: 26905458 Review.
-
Exercise, performance and temperature control: temperature regulation during exercise and implications for sports performance and training.Sports Med. 1985 Jan-Feb;2(1):8-20. doi: 10.2165/00007256-198502010-00002. Sports Med. 1985. PMID: 3883461 Review.
Cited by
-
Genomic regions, candidate genes, and pleiotropic variants associated with physiological and anatomical indicators of heat stress response in lactating sows.BMC Genomics. 2024 May 13;25(1):467. doi: 10.1186/s12864-024-10365-4. BMC Genomics. 2024. PMID: 38741036 Free PMC article.
-
Can Body Mass Index Values and/or Player Position be Viable Predictors for Exertional Heat Illness in American Football Players?Sports Health. 2025 Jul 27:19417381251350670. doi: 10.1177/19417381251350670. Online ahead of print. Sports Health. 2025. PMID: 40717334 Free PMC article.
-
Meta-analysis of heat-induced changes in cardiac function from over 400 laboratory-based heat exposure studies.Nat Commun. 2025 Mar 14;16(1):2543. doi: 10.1038/s41467-025-57868-6. Nat Commun. 2025. PMID: 40087302 Free PMC article.
-
The acute effects of continuous and intermittent whole-body passive heating on cardiovascular disease risk indicators in healthy and young males and females.Eur J Appl Physiol. 2025 Jun;125(6):1591-1606. doi: 10.1007/s00421-025-05718-0. Epub 2025 Feb 14. Eur J Appl Physiol. 2025. PMID: 39953332 Free PMC article.
-
Effects of a Cooling Vest on Core and Skin Temperatures Following a Soccer-Specific Exercise Protocol.Sports (Basel). 2025 Jul 17;13(7):235. doi: 10.3390/sports13070235. Sports (Basel). 2025. PMID: 40711120 Free PMC article.
References
-
- Montain SJ, Coyle EF.. Influence of graded dehydration on hyperthermia and cardiovascular drift during exercise. J Appl Physiol (1985). 1992;73(4):1340–1350. - PubMed
-
- Gonzalez-Alonso J, Mora-Rodriguez R, Below PR, et al. Dehydration reduces cardiac output and increases systemic and cutaneous vascular resistance during exercise. J Appl Physiol (1985). 1995;79(5):1487–1496. - PubMed
-
- Gonzalez-Alonso J, Mora-Rodriguez R, Below PR, et al. Dehydration markedly impairs cardiovascular function in hyperthermic endurance athletes during exercise. J Appl Physiol (1985). 1997;82(4):1229–1236. - PubMed
-
- Trangmar SJ, Gonzalez-Alonso J. New insights into the impact of dehydration on blood flow and metabolism during exercise. Exerc Sport Sci Rev. 2017;45(3):146–153. - PubMed
-
- Rowell LB. Human cardiovascular adjustments to exercise and thermal stress. Physiol Rev. 1974;54(1):75–159. - PubMed
Publication types
LinkOut - more resources
Full Text Sources