

Positive experience with TNF-α inhibitor in toxic epidermal necrolysis resistant to high-dose systemic corticosteroids
- PMID: 37554504
- PMCID: PMC10404849
- DOI: 10.3389/fmed.2023.1210026
Positive experience with TNF-α inhibitor in toxic epidermal necrolysis resistant to high-dose systemic corticosteroids
Abstract
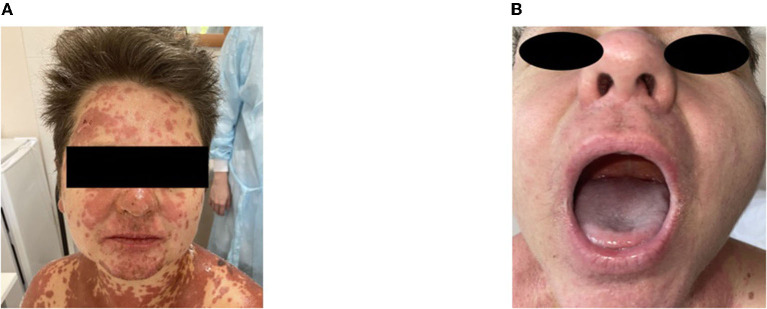
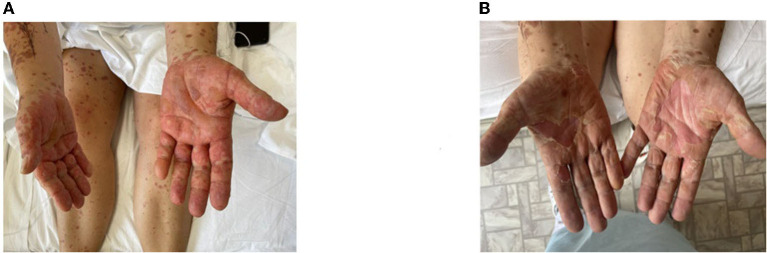
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare, potentially life-threatening syndromes characterized by the development of necrotic epidermal and mucosal lesions. The most common etiologic cause of SJS/TEN is drug-induced mechanisms. The group of drugs with high potential risk includes sulfonamides, anticonvulsants, non-steroidal anti-inflammatory drugs (NSAIDs), allopurinol, phenobarbital, etc. There is no gold standard treatment algorithm for SJS/TEN. In medical practice, systemic glucocorticosteroids (sGCS), intravenous immunoglobulin (IVIG), plasmapheresis, and cyclosporine are used empirically and in various combinations. Recently published studies have demonstrated the efficacy of TNF-α inhibitors as a promising approach in SJS/TEN, including cases resistant to high-dose sGCS, with etanercept and infliximab being the most commonly used drugs. In a large multicenter study by Zhang J et al. (XXXX), 242 patients treated with etanercept, sGCS, or a combination of both had lower mortality compared to the control group. A shorter skin healing time was documented compared to sGCS monotherapy, thus reducing the risk of secondary infections. The published data show a high efficacy with THF-α inhibitor blockade, but the safety of TNF-α inhibitors in patients with SJS/TEN is still questionable due to the paucity of available information. As all clinical research data should be accumulated to provide reliable evidence that the use of TNF-α inhibitors may be beneficial in SJS/TEN, we report a case of etoricoxib-associated SJS with progression to TEN in a 50-year-old woman who was refractory to high-dose sGCS therapy.
Keywords: Etancercept; Stevens-Johnson syndrome; TNF-α inhibitor; TNF-α inhibitor/anti TNF-α; toxic epidermal necrolysis; toxic epidermal necrolysis (Stevens-Johnson syndrome/toxic epidermal necrolysis).
Copyright © 2023 Nikitina, Fomina, Markina, Andreev, Streltsov, Kruglova, Lebedkina, Karaulov and Lysenko.
Conflict of interest statement
EN, DF, UM, SA, YS, TK, MSL, and MAL were employed by SBHI Moscow City Clinical Hospital No. 52 of the Moscow Healthcare Department, and this scientific work was performed as part of their professional responsibilities. The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Evaluation of Combination Therapy With Etanercept and Systemic Corticosteroids for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Multicenter Observational Study.J Allergy Clin Immunol Pract. 2022 May;10(5):1295-1304.e6. doi: 10.1016/j.jaip.2022.01.038. Epub 2022 Feb 4. J Allergy Clin Immunol Pract. 2022. PMID: 35131514
-
Current Perspectives on Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis.Clin Rev Allergy Immunol. 2018 Feb;54(1):147-176. doi: 10.1007/s12016-017-8654-z. Clin Rev Allergy Immunol. 2018. PMID: 29188475 Review.
-
Biologic TNF-α Inhibitors for Stevens-Johnson Syndrome, Toxic Epidermal Necrolysis, and TEN-SJS Overlap: A Study-Level and Patient-Level Meta-Analysis.Dermatol Ther (Heidelb). 2023 Jun;13(6):1305-1327. doi: 10.1007/s13555-023-00928-w. Epub 2023 May 13. Dermatol Ther (Heidelb). 2023. PMID: 37178320 Free PMC article.
-
Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Concise Review with a Comprehensive Summary of Therapeutic Interventions Emphasizing Supportive Measures.Adv Ther. 2017 Jun;34(6):1235-1244. doi: 10.1007/s12325-017-0530-y. Epub 2017 Apr 24. Adv Ther. 2017. PMID: 28439852 Free PMC article. Review.
-
Emerging Insights into Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Induced by Immune Checkpoint Inhibitor and Tumor-Targeted Therapy.J Inflamm Res. 2024 Apr 17;17:2337-2351. doi: 10.2147/JIR.S454673. eCollection 2024. J Inflamm Res. 2024. PMID: 38645875 Free PMC article.
Cited by
-
D-Penicillamine-Induced Stevens-Johnson Syndrome in a Patient with Gold Cyanide Intoxication: A Case Report.Clin Cosmet Investig Dermatol. 2024 Oct 28;17:2409-2415. doi: 10.2147/CCID.S489028. eCollection 2024. Clin Cosmet Investig Dermatol. 2024. PMID: 39494039 Free PMC article.
-
Adalimumab combination with corticosteroid therapy for Stevens-Johnson syndrome/toxic epidermal necrolysis.Arch Dermatol Res. 2025 Apr 10;317(1):694. doi: 10.1007/s00403-025-04214-x. Arch Dermatol Res. 2025. PMID: 40208337 Free PMC article.
-
Toxic epidermal necrolysis following heart transplantation may caused by cefoperazone sodium and sulbactam sodium.J Cardiothorac Surg. 2024 Sep 23;19(1):542. doi: 10.1186/s13019-024-03025-x. J Cardiothorac Surg. 2024. PMID: 39307887 Free PMC article.
References
-
- Seminario-Vidal L, Kroshinsky D, Malachowski SJ, Sun J, Markova A, Beachkofsky TM, et al. . Society of dermatology hospitalists supportive care guidelines for the management of stevens-johnson syndrome/toxic epidermal necrolysis in adults. J Am Acad Dermatol. (2020) 82:1553–67. 10.1016/j.jaad.2020.02.066 - DOI - PubMed
-
- Lysenko MA, Protsenko DN, Fomina DS. Sindrom Stivensa–Dzhonsona i sindrom Lajella u vzroslyh [Stevens-Johnson syndrome and Lyell's syndrome in adults]. Moscow: GEOTAR-Media; 96. [in Russian] (2023).
-
- Schneck J, Fagot JP, Sekula P, Sassolas B, Roujeau JC, Mockenhaupt M. Effects of treatments on the mortality of Stevens-Johnson syndrome and toxic epidermal necrolysis: a retrospective study on patients included in the prospective EuroSCAR study. J Am Acad Dermatol. (2008) 58:33–40. 10.1016/j.jaad.2007.08.039 - DOI - PubMed
-
- Zimmermann S, Sekula P, Venhoff M, Motschall E, Knaus J, Schumacher M, et al. . Systemic immunomodulating therapies for stevens-johnson syndrome and toxic epidermal necrolysis: a systematic review and meta-analysis. JAMA Dermatol. (2017). 153:514–22. 10.1001/jamadermatol.2016.5668 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials