

Oral appliance therapy for obstructive sleep apnea: a retrospective study in a psychiatric sleep clinic
- PMID: 37554945
- PMCID: PMC10405904
- DOI: 10.20407/fmj.2022-023
Oral appliance therapy for obstructive sleep apnea: a retrospective study in a psychiatric sleep clinic
Abstract
Objectives: We evaluated the continuity and effectiveness of oral appliances (OAs) for treating obstructive sleep apnea (OSA) in a psychiatric sleep clinic, specifically focusing on mild cases and those with psychiatric comorbidity.
Methods: We retrospectively examined the medical records of 106 OSA patients treated with OA. Survival analysis was performed to assess the discontinuation of OA use. Clinical Global Impression-Improvement (CGI-I) scale were obtained from medical records. The apnea-hypopnea index (AHI), measured by polysomnography (PSG), and Epworth Sleepiness Scale (ESS) were compared between diagnosis and after post-OA treatment if a second PSG for efficacy assessment was conducted.
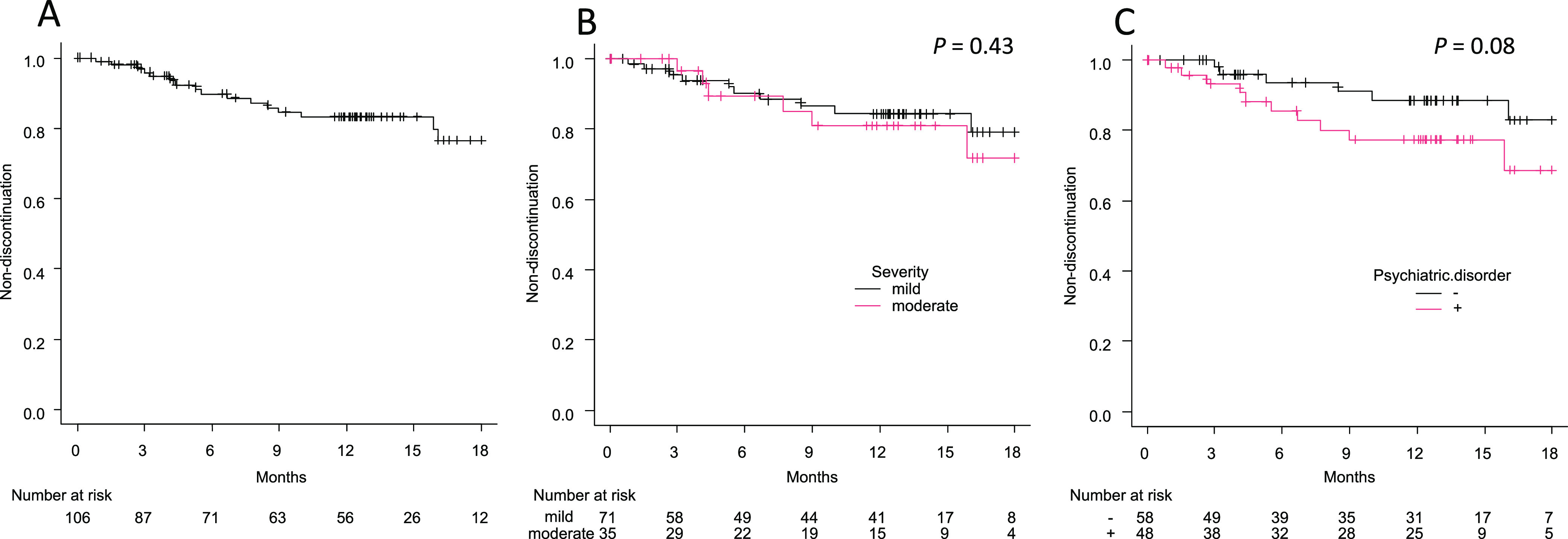
Results: Among all 106 patients, Kaplan-Meier analysis estimated a discontinuation rate of 16.8% at 1 year. This tended to be higher for OSA patients with psychiatric comorbidity (22.7%) than those without (11.6%), though it was not statistically significant (P=0.08). The overall rate of improvement in CGI-I scale was 37.7% and was significantly lower in OSA patients with psychiatric comorbidity (25.0%) than those without (48.3%). Among the 74 patients who underwent a second PSG, AHI and ESS were significantly lower after OA treatment for the entire group and subgroups of OSA severity at diagnosis and psychiatric comorbidity, except for ESS in the moderate OSA severity subgroup.
Conclusion: OA continuation was relatively good, and sleepiness was relieved by OA use, even in mild OSA patients and those with psychiatric comorbidity. However, the continuation and subjective improvement of symptoms were slightly lower in OSA patients with psychiatric comorbidity.
Keywords: Discontinuation; Obstructive sleep apnea; Oral appliance; Psychiatric disorder; Sleepiness.
Conflict of interest statement
The authors have no conflicts of interest to declare related to the present study. MH received personal fees from Dainippon-Sumitomo. NI received research grants from Otsuka, GSK, Tanabe-Mitsubishi, Dainippon-Sumitomo, Eisai, Daiichi Sankyo, Meiji, and received personal fees from Eli Lilly, Janssen, Otsuka, Shionogi, GSK, Dainippon-Sumitomo, Astellas, Yoshitomi, Meiji, Novartis, and Pfizer. TK received research grants from Eisai, Takeda, MSD, and personal fees from Eisai, Tanabe-Mitsubishi, Otsuka, Takeda, Eli Lilly, MSD, Meiji, Yoshitomi Yakuhin, Dainippon-Sumitomo, Fukuda, Shionogi, and Novo Nordisk.
Figures
References
-
- American Academy of Sleep Medicine. International classification of sleep disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014.
-
- Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999; 22: 667–689. - PubMed
-
- Giles TL, Lasserson TJ, Smith BH, White J, Wright J, Cates CJ. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev 2006: CD001106. - PubMed
-
- Fava C, Dorigoni S, Dalle Vedove F, Danese E, Montagnana M, Guidi GC, Narkiewicz K, Minuz P. Effect of CPAP on blood pressure in patients with OSA/hypopnea a systematic review and meta-analysis. Chest 2014; 145: 762–771. - PubMed
-
- Abud R, Salgueiro M, Drake L, Reyes T, Jorquera J, Labarca G. Efficacy of continuous positive airway pressure (CPAP) preventing type 2 diabetes mellitus in patients with obstructive sleep apnea hypopnea syndrome (OSAHS) and insulin resistance: a systematic review and meta-analysis. Sleep Med 2019; 62: 14–21. - PubMed