

Emerging entities: high-grade/large B-cell lymphoma with 11q aberration, large B-cell lymphoma with IRF4 rearrangement, and new molecular subgroups in large B-cell lymphomas. A report of the 2022 EA4HP/SH lymphoma workshop
- PMID: 37555980
- PMCID: PMC10541818
- DOI: 10.1007/s00428-023-03590-x
Emerging entities: high-grade/large B-cell lymphoma with 11q aberration, large B-cell lymphoma with IRF4 rearrangement, and new molecular subgroups in large B-cell lymphomas. A report of the 2022 EA4HP/SH lymphoma workshop
Abstract
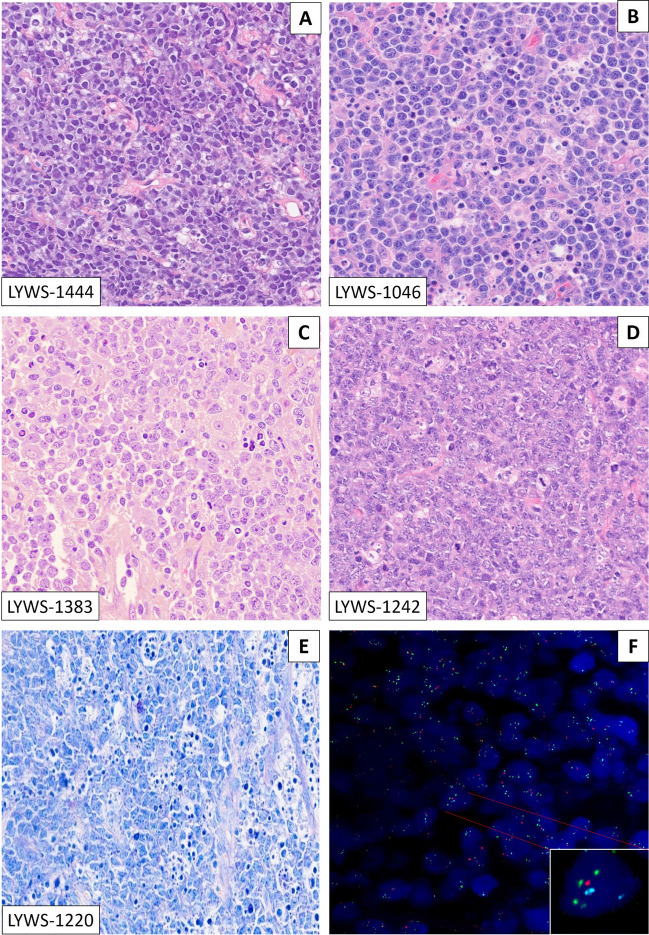
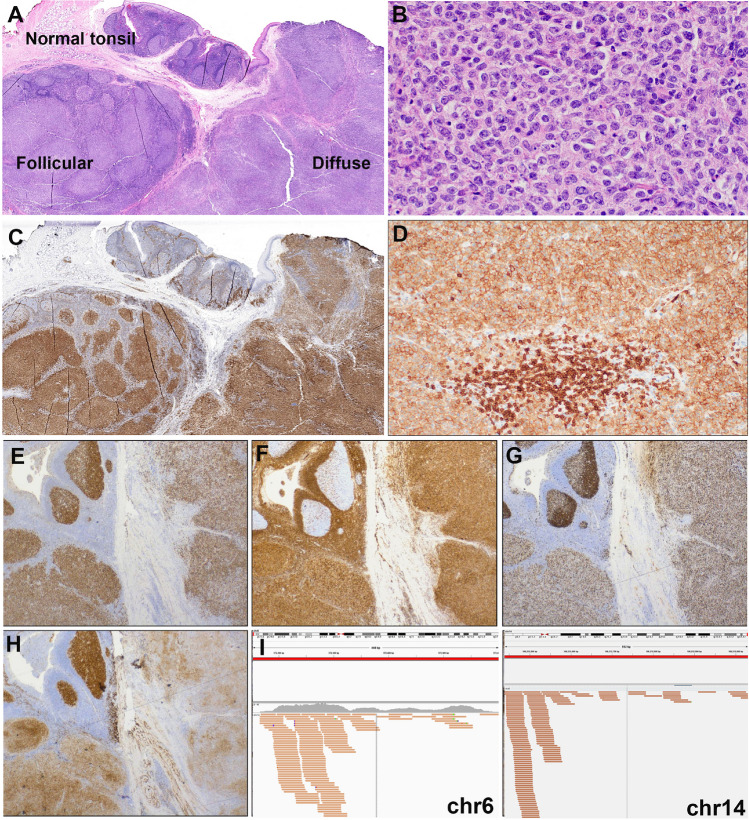
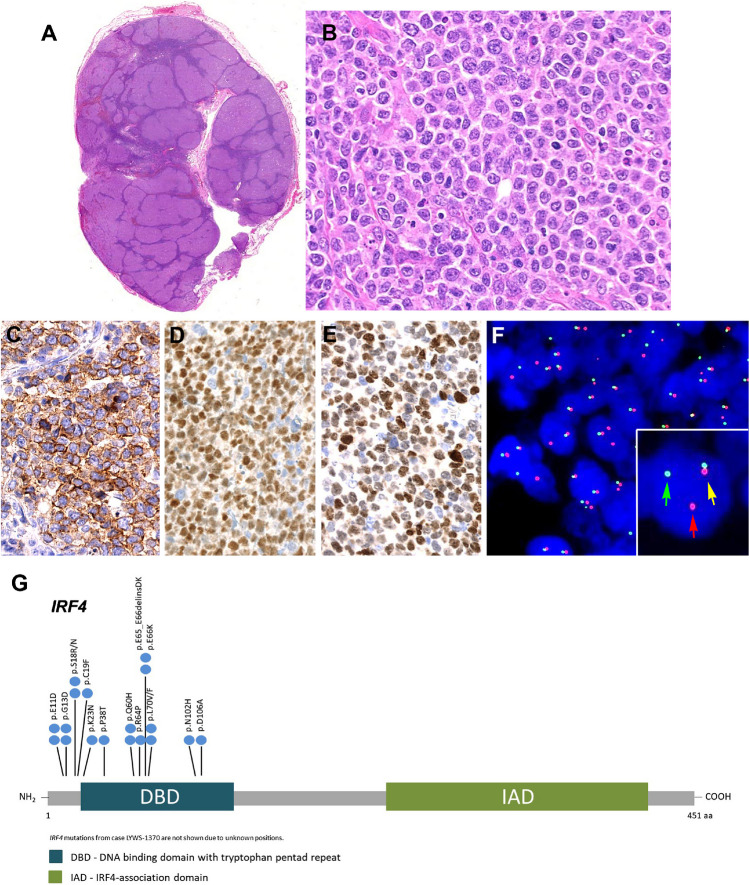
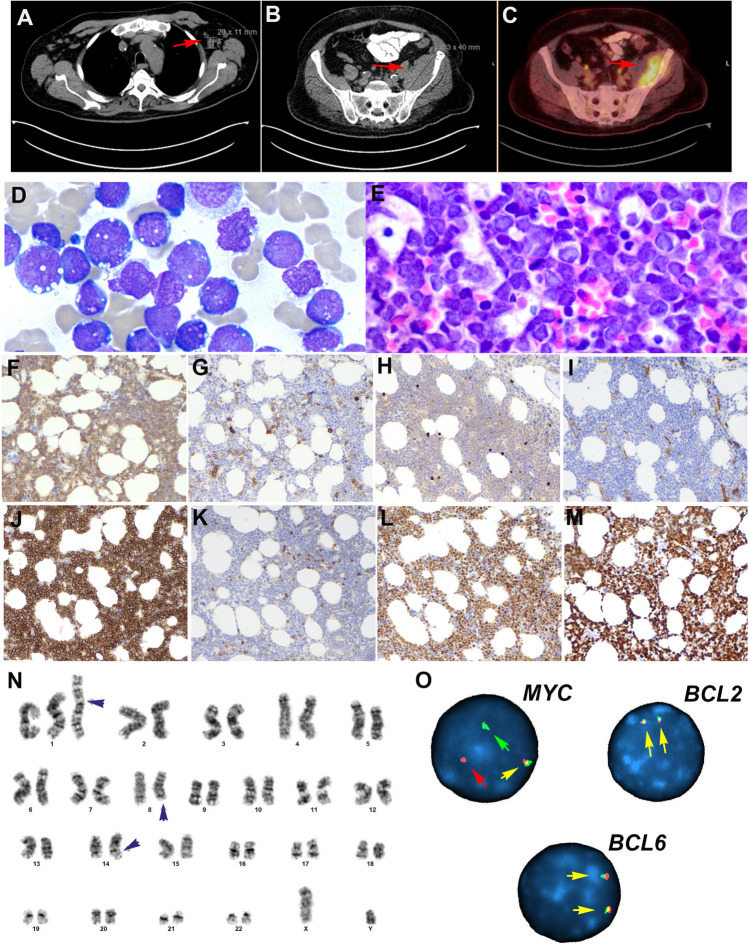
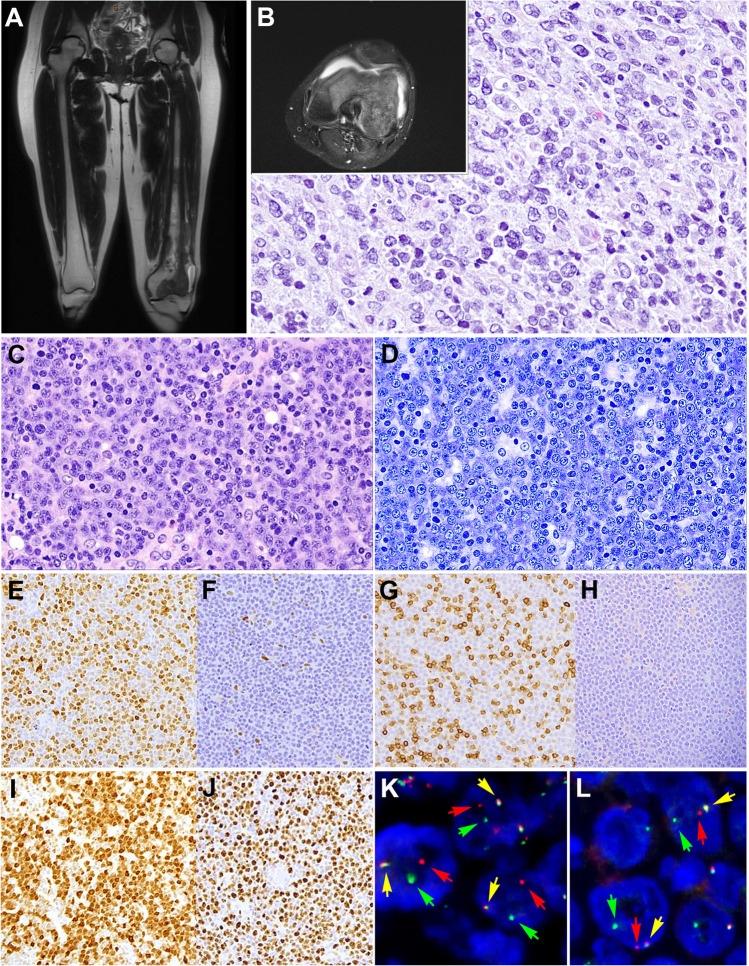
Emerging entities and molecular subgroups in large B-cell lymphomas (LBCLs) were discussed during the 2022 European Association for Haematopathology/Society for Hematopathology workshop in Florence, Italy. This session focused on newly recognized diseases and their diagnostic challenges. High-grade/large B-cell lymphoma with 11q aberration (HG/LBCL-11q) is defined by chromosome 11q-gains and telomeric loss. FISH analysis is recommended for the diagnosis. HG/LBCL-11q can occur in the setting of immunodeficiency, including ataxia-telangiectasia, and predominates in children. The morphological spectrum of these cases is broader than previously thought with often Burkitt-like morphology and coarse apoptotic bodies. It has a Burkitt-like immunophenotype (CD10+, BCL6+, BCL2-) but MYC expression is weak or negative, lacks MYC rearrangement, and is in contrast to Burkitt lymphoma 50% of the cases express LMO2. LBCL with IRF4 rearrangement (LBCL-IRF4) occurs mainly in the pediatric population but also in adults. LBCL-IRF4 has an excellent prognosis, with distinguishing molecular findings. IRF4 rearrangements, although characteristic of this entity, are not specific and can be found in association with other chromosomal translocations in other large B-cell lymphomas. Other molecular subgroups discussed included primary bone diffuse large B-cell lymphoma (PB-DLBCL), which has distinctive clinical presentation and molecular findings, and B-acute lymphoblastic leukemia (B-ALL) with IGH::MYC translocation recently segregated from Burkitt lymphoma with TdT expression. This latter disorder has molecular features of precursor B-cells, often tetrasomy 1q and recurrent NRAS and KRAS mutations. In this report, novel findings, recommendations for diagnosis, open questions, and diagnostic challenges raised by the cases submitted to the workshop will be discussed.
Keywords: 11q aberration; B-ALL with MYC-R; CCND1-R in DLBCL; High-grade/large B-cell lymphoma; IRF4-rearrangement; Plasmablastic transformation; Primary bone lymphoma.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Gascoyne RD, Campo E, Jaffe ES, et al. et al. Diffuse large B-cell lymphoma, NOS. In: Swerdlow SH, Campo E, Harris NL, et al.et al., editors. WHO classification of tumours of haematopoetic and lymphoid tissues. Lyon: International Agency for Research on Cancer; 2017.
-
- Song JY, Dirnhofer S, Piris MA, Quintanilla-Martinez L, Pileri S, Campo E. Diffuse large B-cell lymphomas, not otherwise specified, and emerging entities. Virchows Arch. 2023;482(1):179–192. - PubMed
-
- Alizadeh AA, Eisen MB, Davis RE, et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403(6769):503–511. - PubMed
-
- Pedersen MO, Gang AO, Poulsen TS, et al. MYC translocation partner gene determines survival of patients with large B-cell lymphoma with MYC- or double-hit MYC/BCL2 translocations. Eur J Haematol. 2014;92(1):42–48. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
