

Cavity-based lymphomas: challenges and novel concepts. A report of the 2022 EA4HP/SH lymphoma workshop
- PMID: 37555981
- PMCID: PMC10542738
- DOI: 10.1007/s00428-023-03599-2
Cavity-based lymphomas: challenges and novel concepts. A report of the 2022 EA4HP/SH lymphoma workshop
Erratum in
-
Correction to: Cavity-based lymphomas: challenges and novel concepts. A report of the 2022 EA4HP/SH lymphoma workshop.Virchows Arch. 2023 Sep;483(3):435. doi: 10.1007/s00428-023-03664-w. Virchows Arch. 2023. PMID: 37747560 Free PMC article. No abstract available.
Abstract
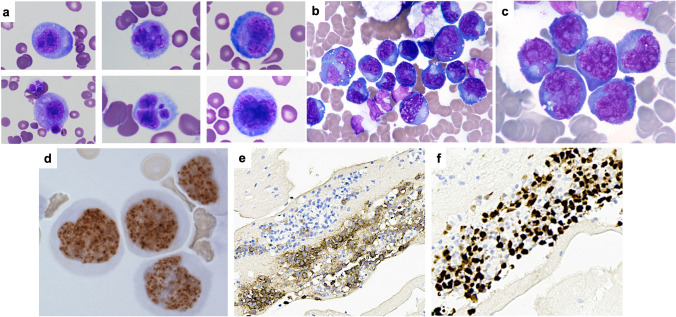
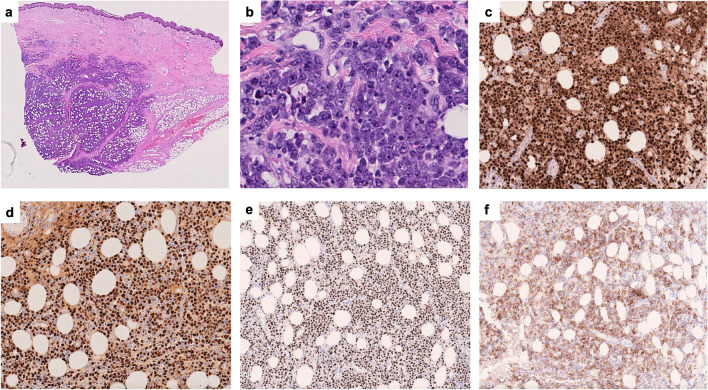
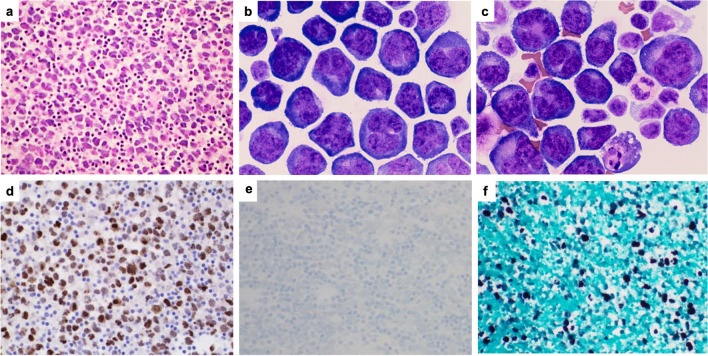
The 2022 European Association for Haematopathology/Society for Hematopathology lymphoma workshop session on cavity-based lymphomas included sixty-eight cases in seven sections. The disease entities discussed include primary effusion lymphomas (PEL), extracavitary primary effusion lymphomas and confounding entities (ECPEL), HHV8-negative B-lineage lymphomas-effusion based (EBV-negative, EBV-positive, and plasmablastic types), diffuse large B-cell lymphoma associated with chronic inflammation, fibrin-associated diffuse large B-cell lymphoma (FA-DLBCL), breast implant-associated anaplastic large cell lymphoma (BIA-ALCL), and other lymphomas presenting as an effusion. All entities above are discussed; however, three are delved into greater detail given the challenges with classification: ECPEL, HHV8-negative effusion-based lymphomas, and FA-DLBCL. Cases exemplifying the diagnostic difficulty in differentiating ECPEL from HHV8-positive diffuse large B-cell lymphoma and germinotropic lymphoproliferative disorder were discussed. The more recently recognized effusion-based HHV8-negative large B-cell lymphoma is explored, with several cases submitted raising the question if this subset should be carved out as a specific entity, and if so, what should be the refining diagnostic criteria. Case submissions to the FA-DLBCL section yielded one of the largest case series to date, including classic cases, cases furthering the discussion on disease sites and prognosis, as well as novel concepts to be considered in this entity. The 2022 EA4HP/SH workshop cases allowed for further confirmation of the characteristics of some of the more historically accepted cavity-based lymphomas, as well as further inquiry and debate on relatively new or evolving entities.
Keywords: Breast Implant associated anaplastic large cell lymphoma; Effusion-based large B cell lymphoma; Extracavitary primary effusion lymphoma; Fibrin-associated large B cell lymphoma; Fluid overload associated large B cell lymphoma; Germinotropic disorder; HHV8-negative effusion lymphoma; Pleural Effusion Lymphoma.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






Similar articles
-
HHV8/KSHV-Positive Lymphoproliferative Disorders and the Spectrum of Plasmablastic and Plasma Cell Neoplasms: 2015 SH/EAHP Workshop Report-Part 3.Am J Clin Pathol. 2017 Feb 1;147(2):171-187. doi: 10.1093/ajcp/aqw218. Am J Clin Pathol. 2017. PMID: 28395104 Free PMC article.
-
Extracavitary/solid variant of primary effusion lymphoma presenting as a gastric mass.Exp Mol Pathol. 2015 Dec;99(3):445-8. doi: 10.1016/j.yexmp.2015.09.010. Epub 2015 Sep 25. Exp Mol Pathol. 2015. PMID: 26407759
-
Epstein-Barr virus reactivation influences clonal evolution in human herpesvirus-8-related lymphoproliferative disorders.Histopathology. 2021 Dec;79(6):1099-1107. doi: 10.1111/his.14551. Epub 2021 Oct 4. Histopathology. 2021. PMID: 34431125 Free PMC article.
-
Lymphomas arising in immune-privileged sites: insights into biology, diagnosis, and pathogenesis.Virchows Arch. 2020 May;476(5):647-665. doi: 10.1007/s00428-019-02698-3. Epub 2019 Dec 20. Virchows Arch. 2020. PMID: 31863183 Review.
-
Emerging entities: high-grade/large B-cell lymphoma with 11q aberration, large B-cell lymphoma with IRF4 rearrangement, and new molecular subgroups in large B-cell lymphomas. A report of the 2022 EA4HP/SH lymphoma workshop.Virchows Arch. 2023 Sep;483(3):281-298. doi: 10.1007/s00428-023-03590-x. Epub 2023 Aug 9. Virchows Arch. 2023. PMID: 37555980 Free PMC article. Review.
Cited by
-
Rapid On-Site Cytologic Evaluation-Facilitated Diagnosis of Fibrin-Associated Large B-Cell Lymphoma in a Right Atrial Fibrin Thrombus: A Case Report.Case Rep Oncol. 2025 Jun 13;18(1):965-971. doi: 10.1159/000546869. eCollection 2025 Jan-Dec. Case Rep Oncol. 2025. PMID: 40672718 Free PMC article.
-
Promising immunotherapeutic approaches for primary effusion lymphoma.Explor Target Antitumor Ther. 2024;5(3):699-713. doi: 10.37349/etat.2024.00242. Epub 2024 Jun 26. Explor Target Antitumor Ther. 2024. PMID: 38966176 Free PMC article. Review.
-
Fibrin associated large B-cell lymphoma accidentally identified in a breast implant capsule: a molecular report of a rare entity.Pathologica. 2024 Aug;116(4):242-248. doi: 10.32074/1591-951X-944. Pathologica. 2024. PMID: 39377506 Free PMC article.
-
Emerging Non-Breast Implant-Associated Lymphomas: A Systematic Review.Cancers (Basel). 2024 Dec 5;16(23):4085. doi: 10.3390/cancers16234085. Cancers (Basel). 2024. PMID: 39682271 Free PMC article.
-
The Possible Role of Pathogens and Chronic Immune Stimulation in the Development of Diffuse Large B-Cell Lymphoma.Biomedicines. 2024 Mar 14;12(3):648. doi: 10.3390/biomedicines12030648. Biomedicines. 2024. PMID: 38540261 Free PMC article. Review.
References
-
- Steven H, Swerdlow EC, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Arber DA, Hasserjian RP, Le Beau MM, Orazi A, Siebert R. WHO classification of tumours of haematopoietic and lymphoid tissues (Revised 4th Edition) Lyon: IARC; 2017.
-
- King RL, Goodlad JR, Calaminici M, et al. Lymphomas arising in immune-privileged sites: insights into biology, diagnosis, and pathogenesis. Virchows Arch. 2020;476(5):647–665. - PubMed
