

Coronary Angiography After Out-of-Hospital Cardiac Arrest Without ST-Segment Elevation: One-Year Outcomes of a Randomized Clinical Trial
- PMID: 37556123
- PMCID: PMC10413219
- DOI: 10.1001/jamacardio.2023.2264
Coronary Angiography After Out-of-Hospital Cardiac Arrest Without ST-Segment Elevation: One-Year Outcomes of a Randomized Clinical Trial
Abstract
Importance: Myocardial infarction is a frequent cause of out-of-hospital cardiac arrest (OHCA). The long-term effect of early coronary angiography on patients with OHCA with possible coronary trigger but no ST-segment elevation remains unclear.
Objective: To compare the clinical outcomes of early unselective angiography with the clinical outcomes of a delayed or selective approach for successfully resuscitated patients with OHCA of presumed cardiac origin without ST-segment elevation at 1-year follow-up.
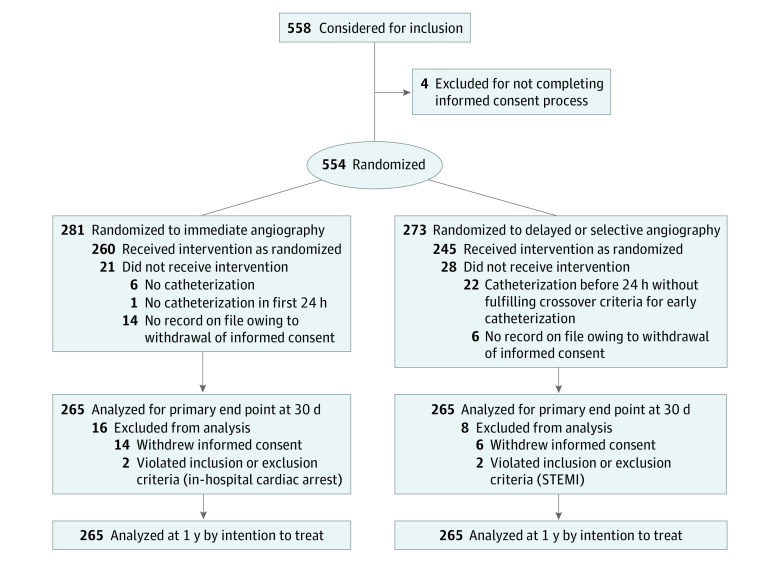
Design, setting, and participants: The TOMAHAWK trial was a multicenter, international (Germany and Denmark), investigator-initiated, open-label, randomized clinical trial enrolling 554 patients between November 23, 2016, to September 20, 2019. Patients with stable return of spontaneous circulation after OHCA of presumed cardiac origin but without ST-segment elevation on the postresuscitation electrocardiogram were eligible for inclusion. A total of 554 patients were randomized to either immediate coronary angiography after hospital admission or an initial intensive care assessment with delayed or selective angiography after a minimum of 24 hours. All 554 patients were included in survival analyses during the follow-up period of 1 year. Secondary clinical outcomes were assessed only for participants alive at 1 year to account for the competing risk of death.
Interventions: Early vs delayed or selective coronary angiography and revascularization if indicated.
Main outcomes and measures: Evaluations in this secondary analysis included all-cause mortality after 1 year, as well as severe neurologic deficit, myocardial infarction, and rehospitalization for congestive heart failure in survivors at 1 year.
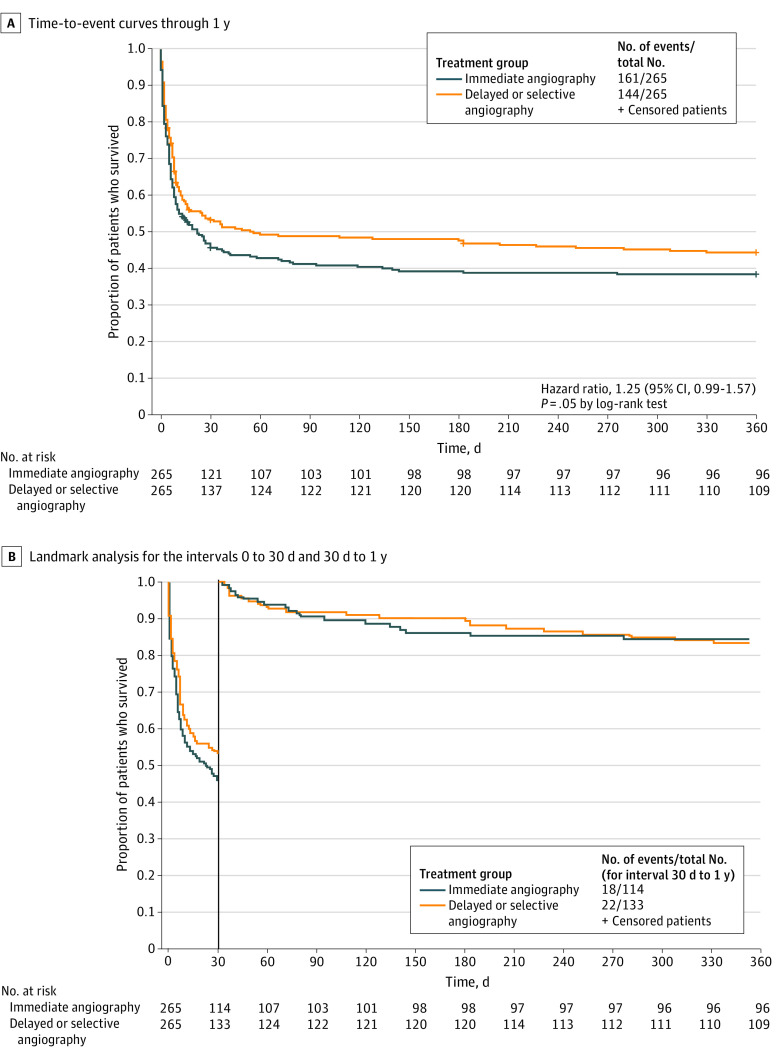
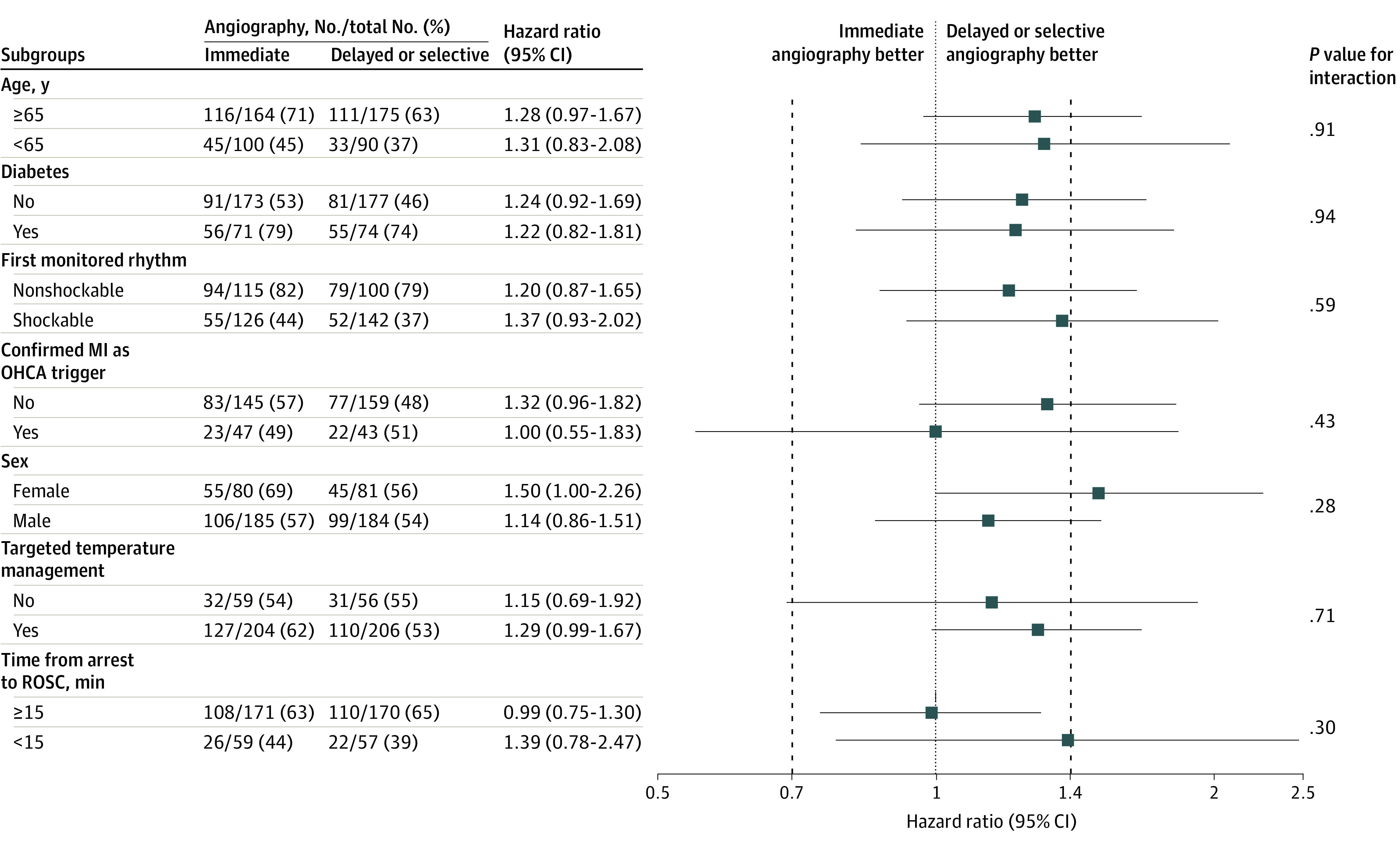
Results: A total of 281 patients were randomized to the immediate angiography group and 273 to the delayed or selective group, with a median age of 70 years (IQR, 60-78 years). A total of 369 of 530 patients (69.6%) were male, and 268 of 483 patients (55.5%) had a shockable arrest rhythm. At 1 year, all-cause mortality was 60.8% (161 of 265) in the immediate angiography group and 54.3% (144 of 265) in the delayed or selective angiography group without significant difference between the treatment strategies, trending toward an increase in mortality with immediate angiography (hazard ratio, 1.25; 95% CI, 0.99-1.57; P = .05). For patients surviving until 1 year, the rates of severe neurologic deficit, myocardial infarction, and rehospitalization for congestive heart failure were similar between the groups.
Conclusions and relevance: This study found that a strategy of immediate coronary angiography does not provide clinical benefit compared with a delayed or selective invasive approach for patients 1 year after resuscitated OHCA of presumed coronary cause and without ST-segment elevation.
Trial registration: ClinicalTrials.gov Identifier: NCT02750462.
Conflict of interest statement
Figures
Comment in
-
Out-of-Hospital Cardiac Arrest-One Size Does Not Fit All.JAMA Cardiol. 2023 Sep 1;8(9):835-836. doi: 10.1001/jamacardio.2023.2277. JAMA Cardiol. 2023. PMID: 37556149 No abstract available.
References
-
- Ibanez B, James S, Agewall S, et al. ; ESC Scientific Document Group . 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119-177. doi:10.1093/eurheartj/ehx393 - DOI - PubMed
-
- Dumas F, Cariou A, Manzo-Silberman S, et al. . Immediate percutaneous coronary intervention is associated with better survival after out-of-hospital cardiac arrest: insights from the PROCAT (Parisian Region Out of Hospital Cardiac Arrest) registry. Circ Cardiovasc Interv. 2010;3(3):200-207. doi:10.1161/CIRCINTERVENTIONS.109.913665 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
