

10-channel phased-array coil for carotid wall MRI at 3T
- PMID: 37556496
- PMCID: PMC10411804
- DOI: 10.1371/journal.pone.0288529
10-channel phased-array coil for carotid wall MRI at 3T
Abstract
Background: Accurate assessment of plaque accumulation near the carotid bifurcation is important for the effective prevention and treatment of stroke. However, vessel and plaque delineation using MRI can be limited by low contrast-to-noise ratio (CNR) and long acquisition times. In this work, a 10-channel phased-array receive coil design for bilateral imaging of the carotid bifurcation using 3T MRI is proposed.
Methods: The proposed 10-channel receive coil was compared to a commercial 4-channel receive coil configuration using data acquired from phantoms and healthy volunteers (N = 9). The relative performance of the coils was assessed, by comparing signal-to-noise ratio (SNR), noise correlation, g-factor noise amplification, and the CNR between vessel wall and lumen using black-blood sequences. Patient data were acquired from 12 atherosclerotic carotid artery disease patients.
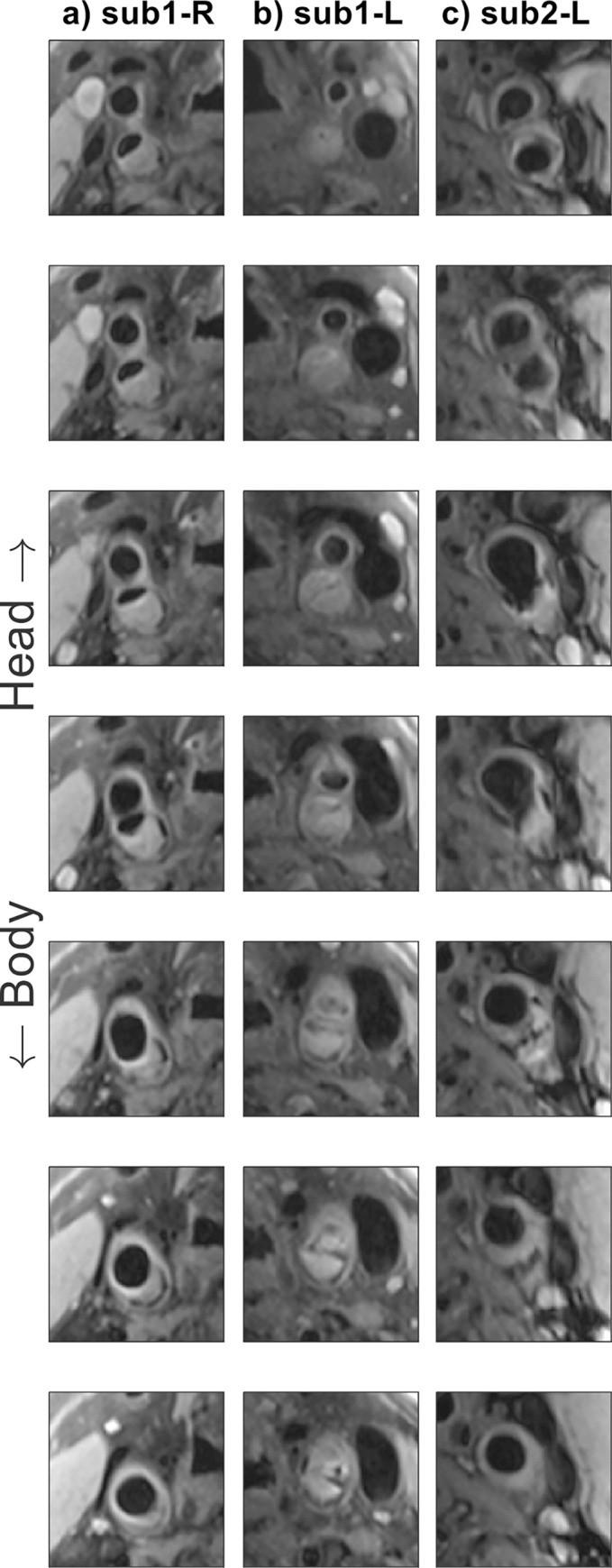
Results: The 10-channel coil consistently provided substantially increased SNR in phantoms (+77 ± 27%) and improved CNR in healthy carotid arteries (+62 ± 11%), or reduced g-factor noise amplification. Patient data showed excellent delineation of atherosclerotic plaque along the length of the carotid bifurcation using the 10-channel coil.
Conclusions: The proposed 10-channel coil design allows for improved visualization of the carotid arteries and the carotid bifurcation and increased parallel imaging acceleration factors relative to a commercial 4-channel coil design.
Copyright: © 2023 de Buck et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: MdB receives studentship support from Siemens Healthineers and CR is an employee of PulseTeq Limited. We confirm that our competing interests do not alter our adherence to PLOS ONE policies on sharing data and materials, and have included this in the cover letter as requested.
Figures






References
-
- Masaryk TJ, Ross JS, Modic MT, Lenz GW, Haacke EM. Carotid Bifurcation: MR Imaging. Neuroradiology. 1988;166: 461–466. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
