

Association between vaginal microbiomes and neonatal septicemia in pregnant women with preterm premature rupture of membranes based on metagenome sequencing
- PMID: 37560239
- PMCID: PMC10408501
Association between vaginal microbiomes and neonatal septicemia in pregnant women with preterm premature rupture of membranes based on metagenome sequencing
Abstract
Background: Preterm premature rupture of membranes (PPROM) is closely associated with pathogenic microbiomes in the female reproductive tract, and can lead to neonatal septicemia. The current study aimed to investigate potential pathogenic microbiomes associated with neonatal septicemia based on DNA metagenome sequencing.
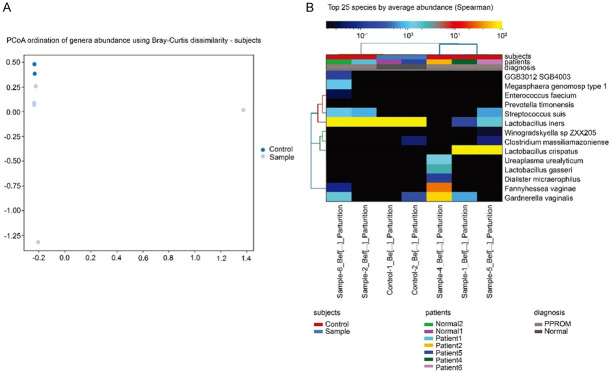
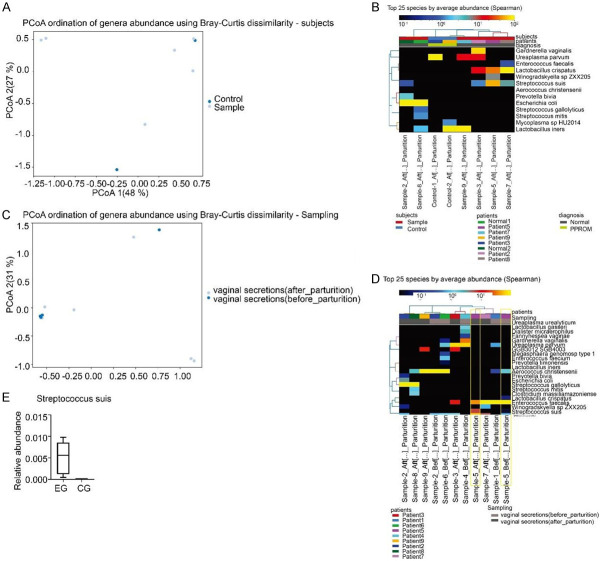
Methods: In this study, a total of 7 pregnant women with PPROM presenting neonatal septicemia (experimental group) and 3 pregnant women with normal newborns (control group) were enrolled. Vaginal secretions at admission and before parturition as well as placental tissues after parturition were collected for DNA metagenome sequencing using whole genome shotgun method on the Illumina NovaSeq/HiSeq platform. Raw data were processed by BioBakery workflow, and MetaPhlAn4 was implemented for qualitative and quantitative analyses of microbiome. Lactobacillus crispatus, Gardneralla vaginalis, Fannyhessea vaginae and Streptococcus suis were specifically detected from the experimental group. The two groups were compared using Student's t-tests.
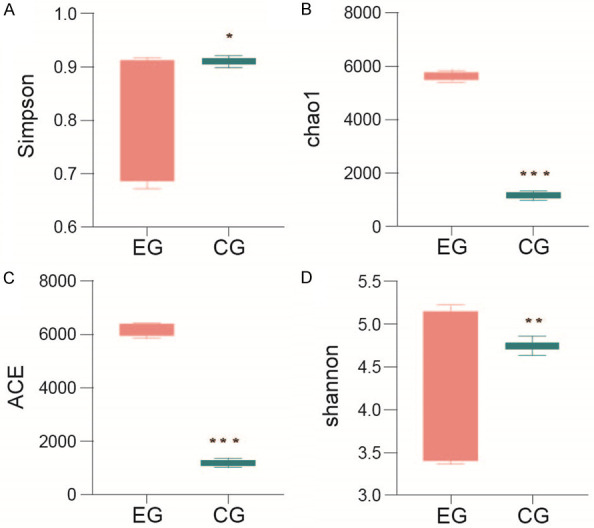
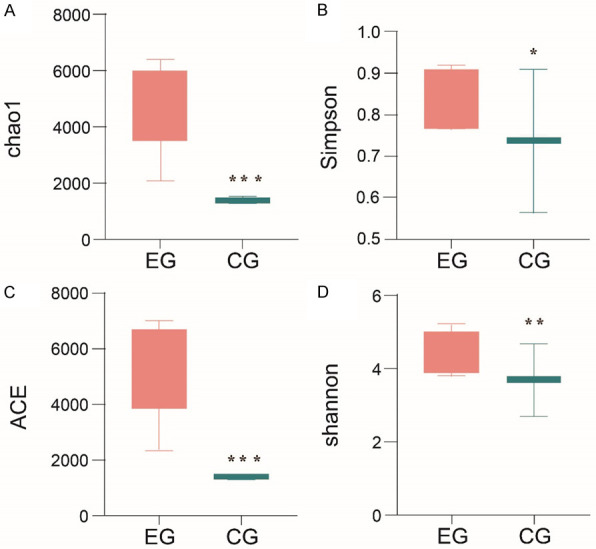
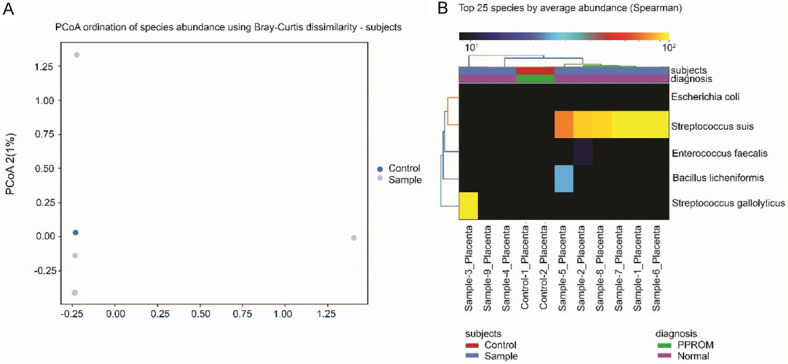
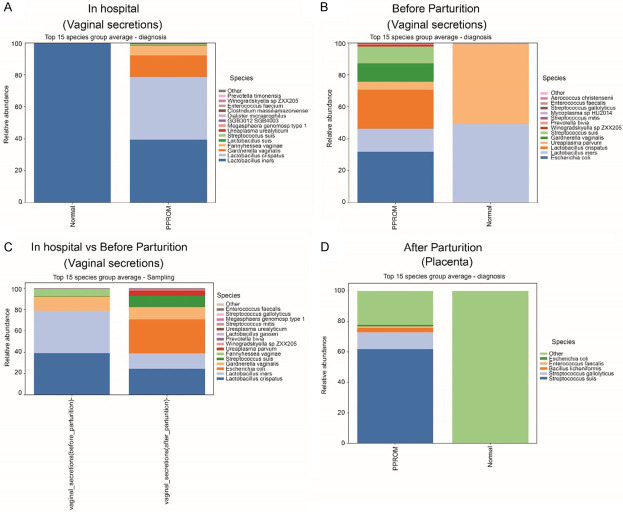
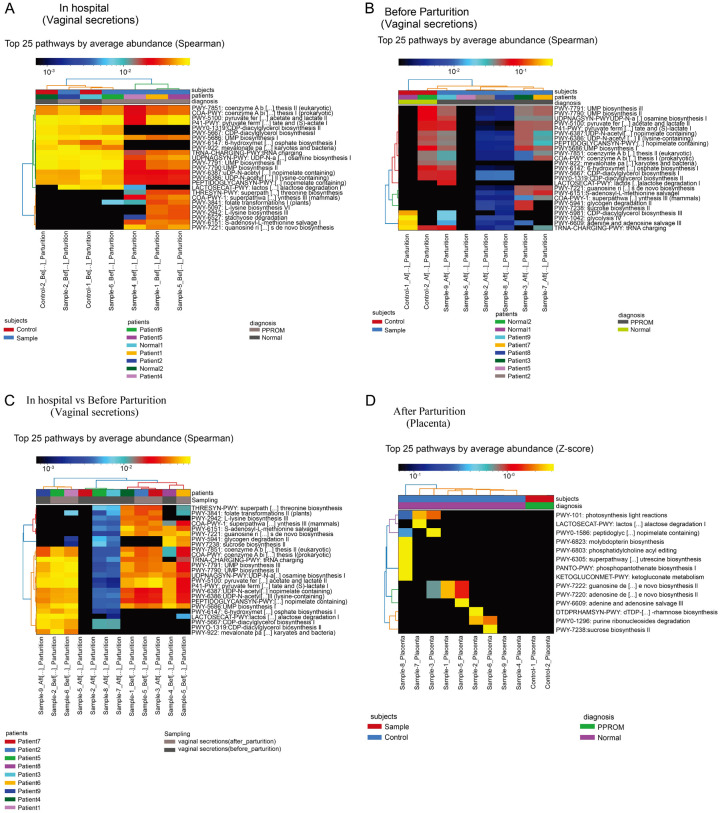
Results: The indexes of Chao1 (P=0.00028/P=0.00072), abundance-based coverage estimator (ACE, P=0.00059/P=0.00026), Shannon (P=0.036/P=0.0065) and Simpson (P=0.007/P=0.041) in the experimental group were increased at admission and before parturition as compared with the control group. Several microbiomes, such as Lactobacillus crispatus, Gardneralla vaginalis, Fannyhessea vaginae and Streptococcus suis, were specifically detected in the experimental group. Notably, Gardnerella vaginalis and Streptococcus gallolyticus were identified from the vaginal secretions and placenta tissues of women with neonatal septicemia. Moreover, nucleic acid synthesis and carbohydrate metabolism-related pathways were enriched in the experimental group.
Conclusion: This study enhanced the current understanding of the mechanisms underlying pathogenic microbiomes in PPROM-induced neonatal septicemia. The trial registry number is ChiCTR2300070666 (URL: https://www.chictr.org.cn/showproj.html?proj=195648).
Keywords: Preterm premature rupture of membranes; metabolic pathways; microbiomes; neonatal septicemia; whole genome shotgun.
AJTR Copyright © 2023.
Conflict of interest statement
None.
Figures
References
-
- Medina TM, Hill DA. Preterm premature rupture of membranes: diagnosis and management. Am Fam Physician. 2006;73:659–664. - PubMed
-
- Lee WL, Chang WH, Wang PH. Risk factors associated with preterm premature rupture of membranes (PPROM) Taiwan J Obstet Gynecol. 2021;60:805–806. - PubMed
-
- Chiossi G, Di Tommaso M, Monari F, Consonni S, Strambi N, Zoccoli SG, Seravalli V, Comerio C, Betti M, Cappello A, Vergani P, Facchinetti F, Locatelli A. Neonatal outcomes and risk of neonatal sepsis in an expectantly managed cohort of late preterm prelabor rupture of membranes. Eur J Obstet Gynecol Reprod Biol. 2021;261:1–6. - PubMed
-
- Velemínský M Jr, Stránský P, Velemínský M Sr, Tosner J. Relationship of IL-6, IL-8, TNF and sICAM-1 levels to PROM, pPROM, and the risk of early-onset neonatal sepsis. Neuro Endocrinol Lett. 2008;29:303–311. - PubMed
-
- Mikołajczyk M, Wirstlein P, Adamczyk M, Skrzypczak J, Wender-Ożegowska E. Value of cervicovaginal fluid cytokines in prediction of fetal inflammatory response syndrome in pregnancies complicated with preterm premature rupture of membranes (pPROM) J Perinat Med. 2020;48:249–255. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous