

Atypical Hemolytic-Uremic Syndrome: Genetic Basis, Clinical Manifestations, and a Multidisciplinary Approach to Management
- PMID: 37560408
- PMCID: PMC10408684
- DOI: 10.2147/JMDH.S245620
Atypical Hemolytic-Uremic Syndrome: Genetic Basis, Clinical Manifestations, and a Multidisciplinary Approach to Management
Abstract
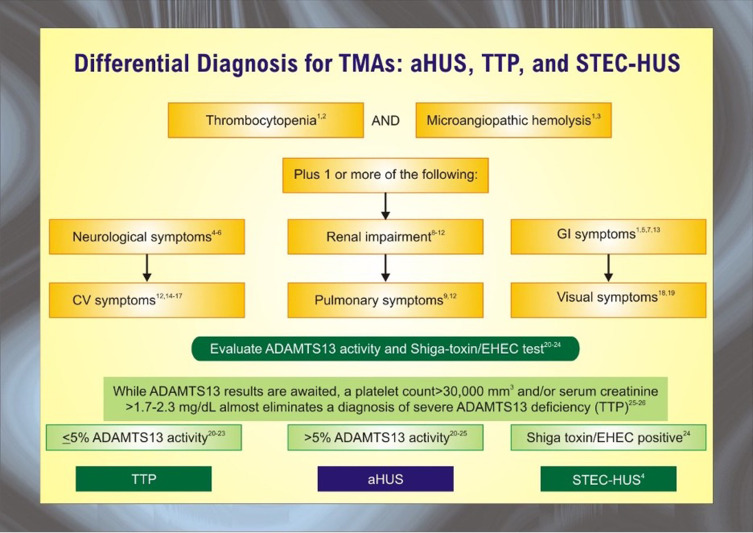
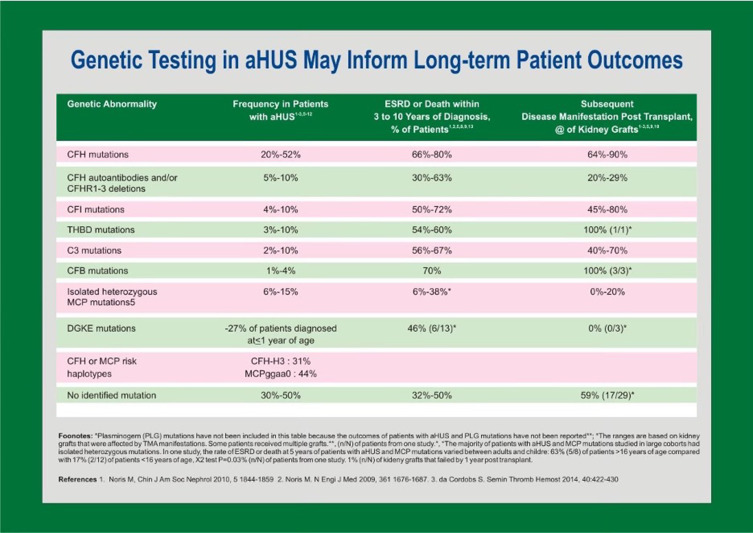
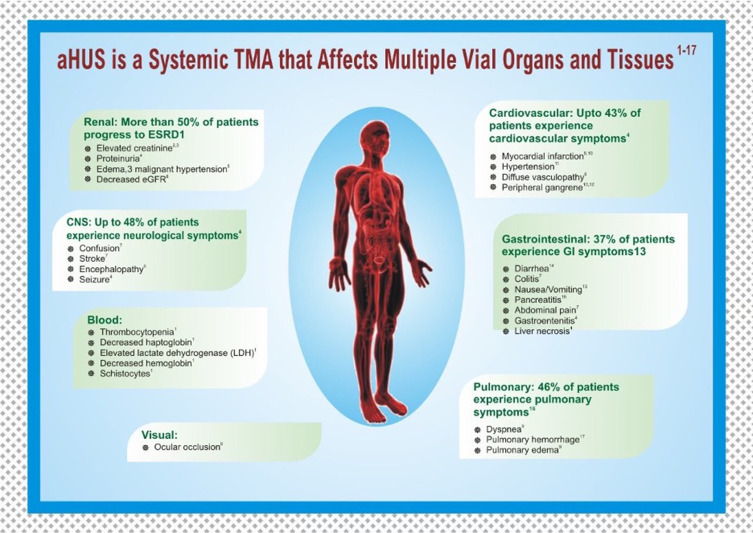
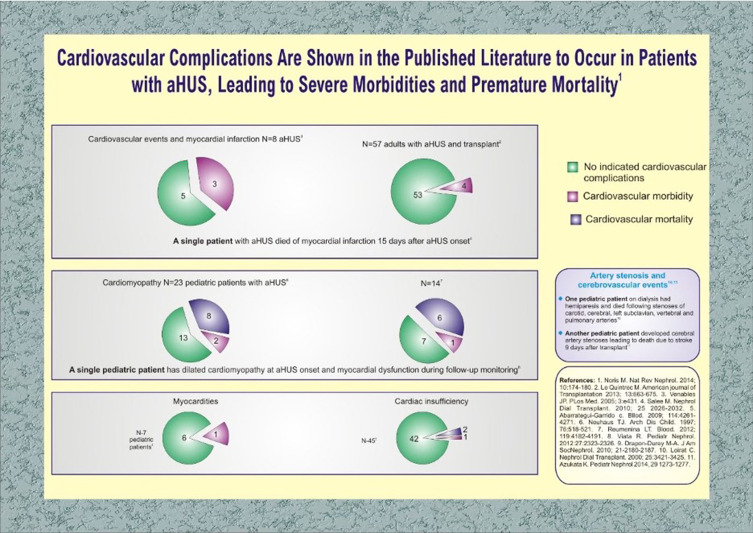
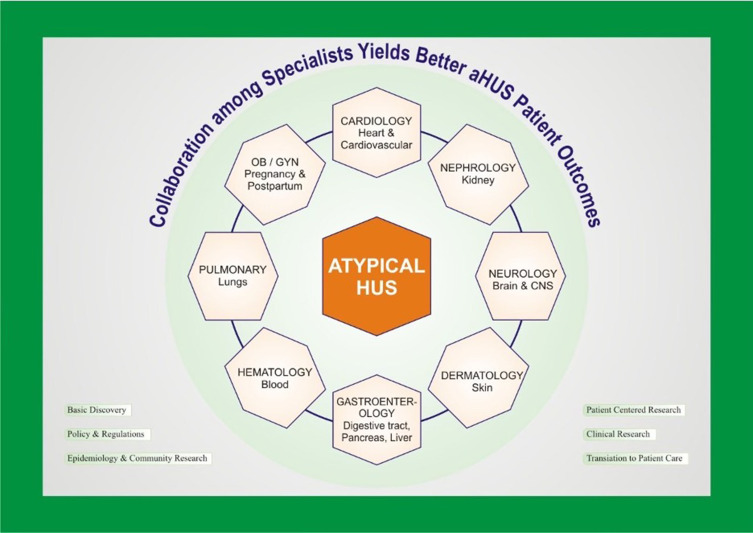
Hemolytic uremic syndrome (HUS) is a thrombotic microangiopathy (TMA) defined by the triad of hemolytic anemia, thrombocytopenia, and acute kidney injury. Microthrombi develop in the glomerular capillaries secondary to endothelial damage and exert shear stress on red blood cells, consume platelets, and contribute to renal dysfunction and failure. Per current understanding of pathophysiology, HUS is classified into infectious, secondary, and atypical disease. The most common etiology is infectious sequelae of Shiga toxin-producing Escherichia coli (STEC); other causative organisms include shigella and salmonella. Secondary HUS arises from cancer, chemotherapy, solid organ and hematopoietic stem cell transplant, pregnancy, or autoimmune disorders. Primary atypical hemolytic-uremic syndrome (aHUS) is associated with genetic mutations in complement and complement regulatory proteins. Under physiologic conditions, complement regulators keep the alternative complement system continuously active at low levels. In times of inflammation, mutations in complement-related proteins lead to uncontrolled complement activity. The hyperactive inflammatory state leads to glomerular endothelial damage, activation of the coagulation cascade, and TMA findings. Atypical hemolytic-uremic syndrome is a rare disorder with a prevalence of 2.21 to 9.4 per million people aged 20 years or younger; children between the ages of 0 and 4 are most affected. Multidisciplinary health care is necessary for timely management of its extra-renal manifestations. These include vascular disease of the heart, brain, and skin, pulmonary hypertension and hemorrhage, and pregnancy complications. Adequate screening is required to monitor for sequelae. First-line treatment is the monoclonal antibody eculizumab, but several organ systems may require specialized interventions and coordination of care with sub-specialists.
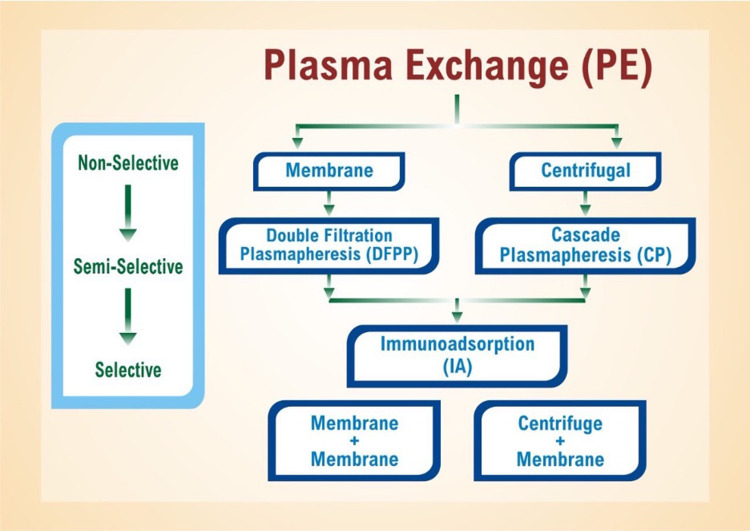
Keywords: atypical hemolytic uremic syndrome; complications; eculizumab; extra-renal manifestations; plasma exchange.
© 2023 Yerigeri et al.
Conflict of interest statement
Prof. Dr. Olivia Boyer reports personal fees from Alexion, during the conduct of the study; personal fees from Alnylam, CSL/Vifor, and Purespring, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
References
-
- Janeway CA, Travers P, Walport M, et al. Immunobiology: the immune system in health and disease. In: The Complement System and Innate Immunity. 5th ed. New York: Garland Science;2001. Available from: www.ncbi.nlm.nih.gov/books/NBK27100/.
Publication types
LinkOut - more resources
Full Text Sources
Medical
