

Scientific opinion on the tolerable upper intake level for vitamin D, including the derivation of a conversion factor for calcidiol monohydrate
- PMID: 37560437
- PMCID: PMC10407748
- DOI: 10.2903/j.efsa.2023.8145
Scientific opinion on the tolerable upper intake level for vitamin D, including the derivation of a conversion factor for calcidiol monohydrate
Abstract
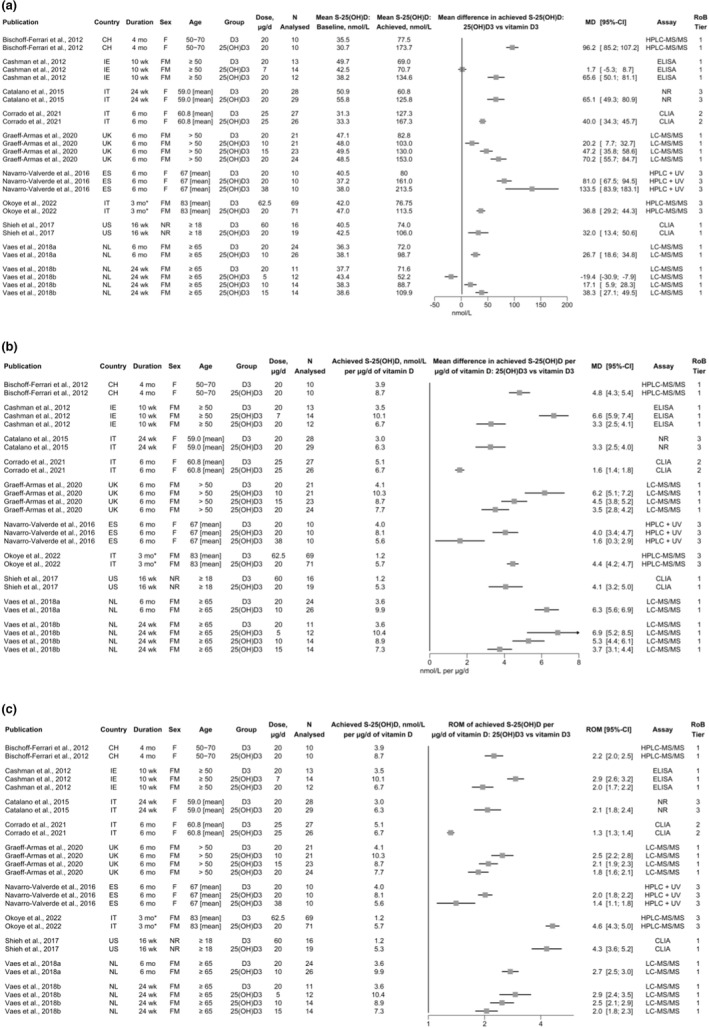
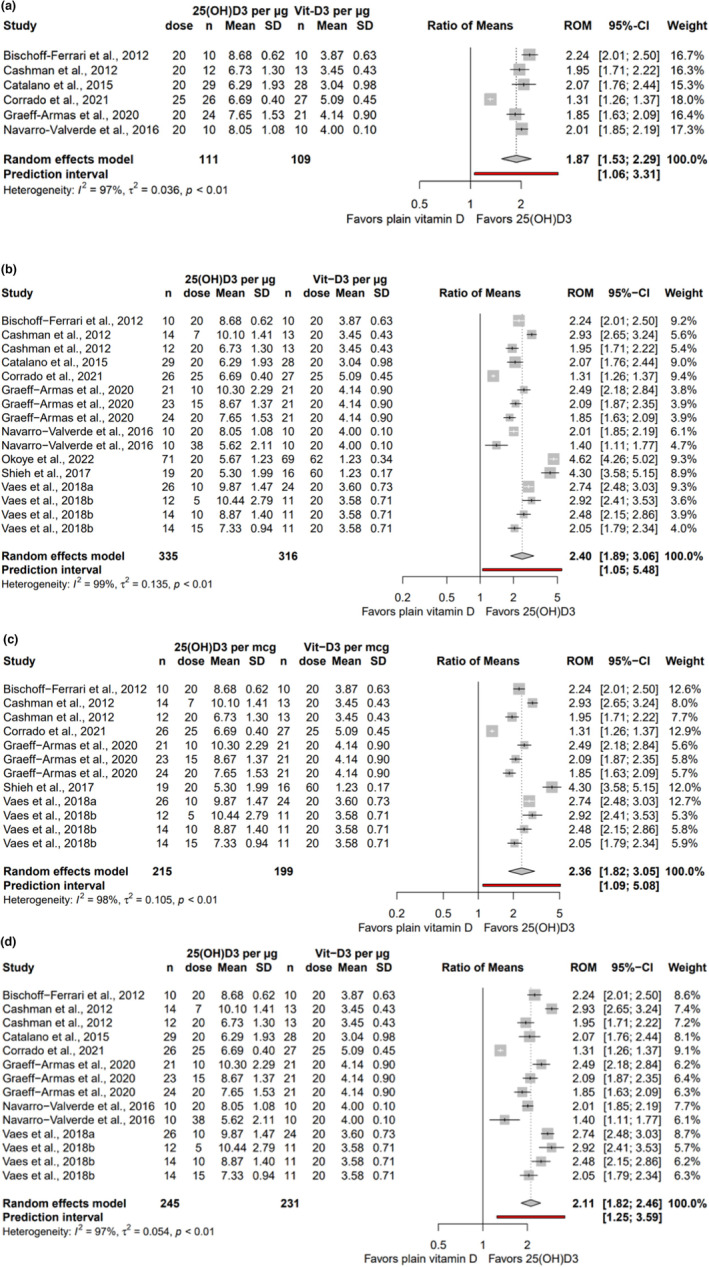
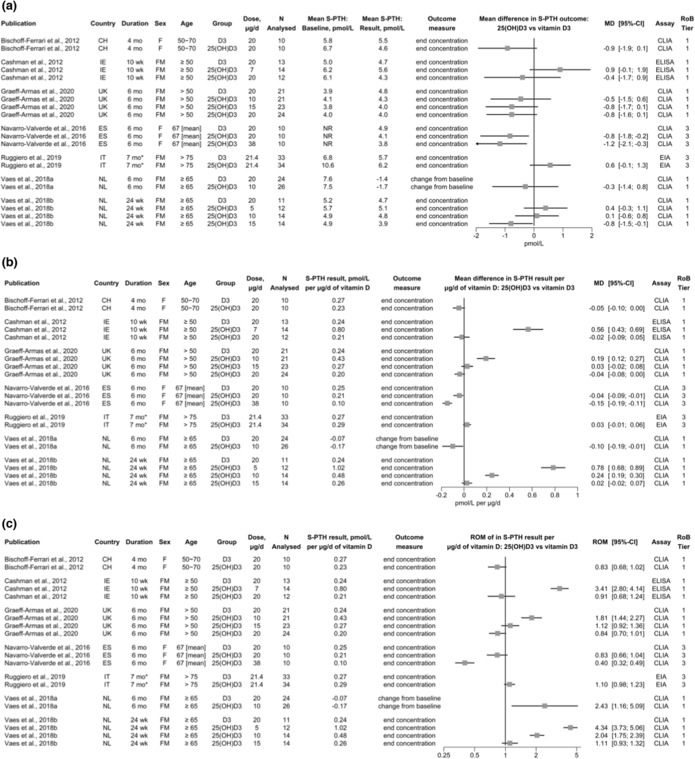
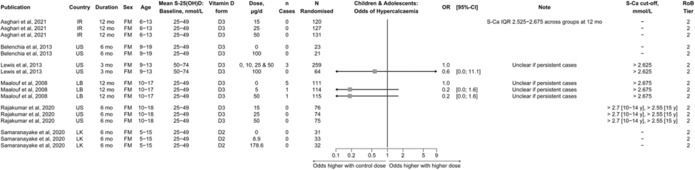
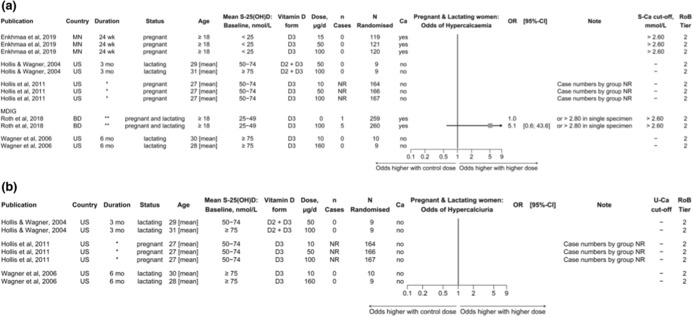
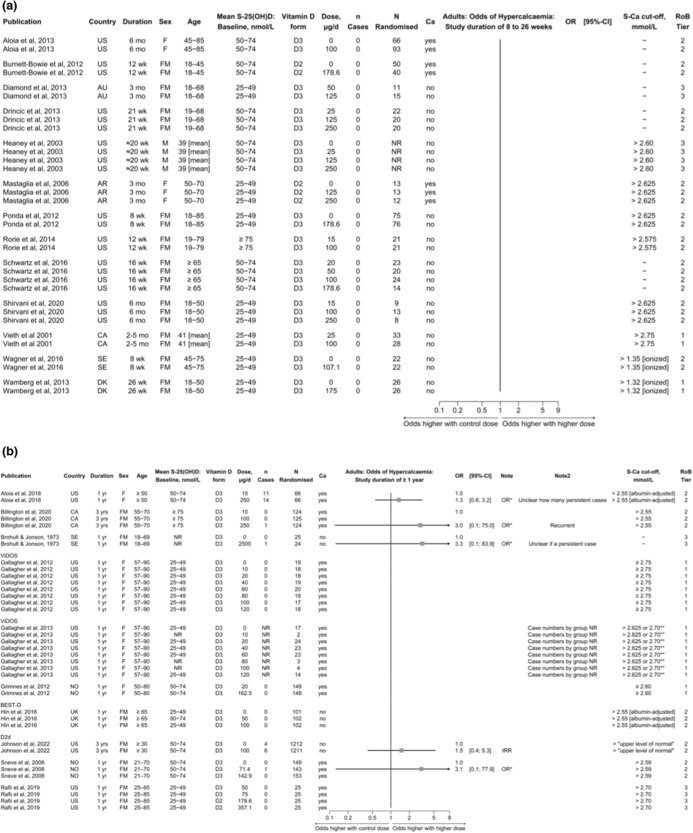
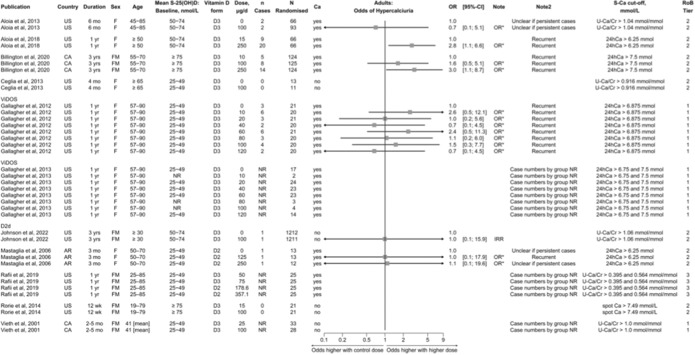
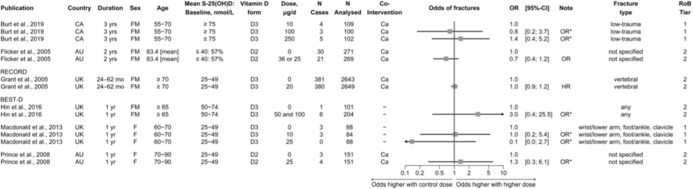
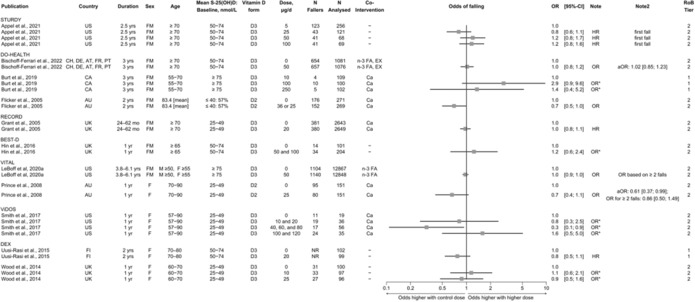
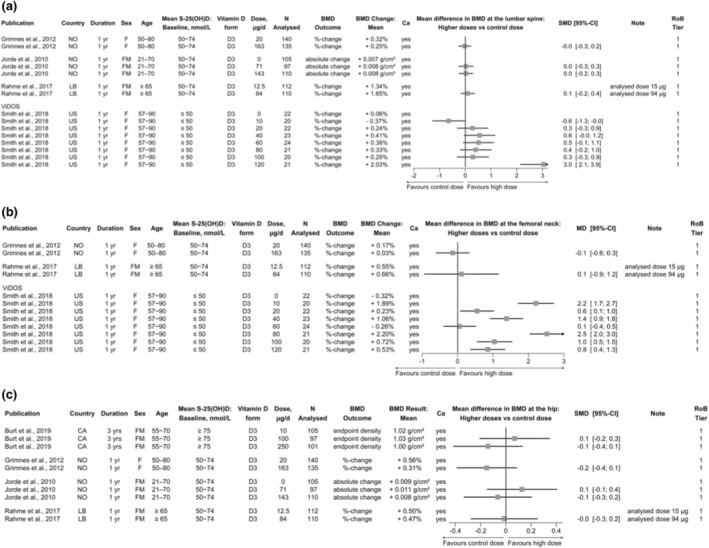
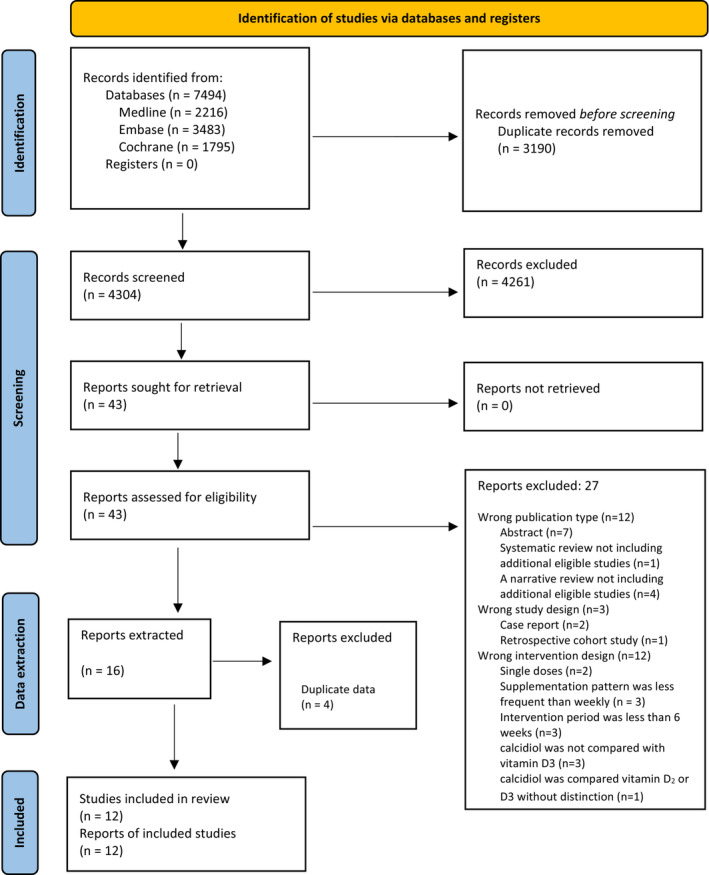
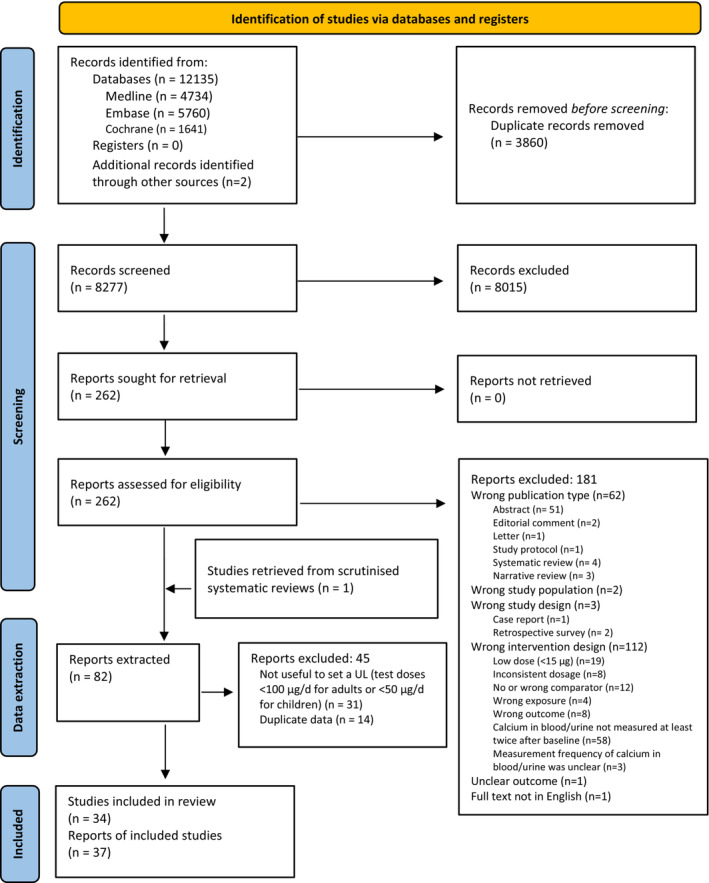
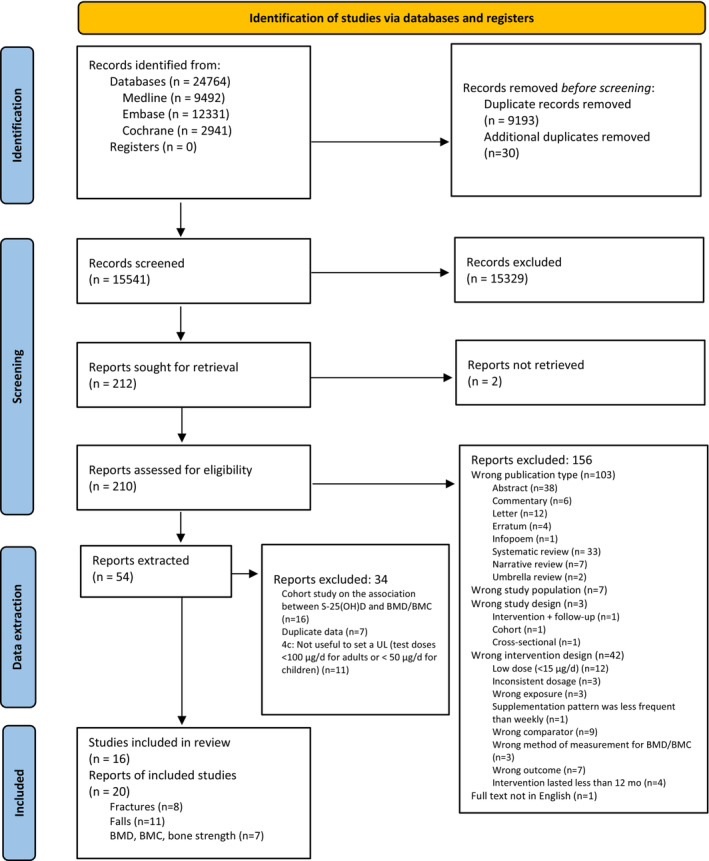
Following two requests from the European Commission (EC), the EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA) was asked to deliver a scientific opinion on the revision of the tolerable upper intake level (UL) for vitamin D and to propose a conversion factor (CF) for calcidiol monohydrate into vitamin D3 for labelling purposes. Vitamin D refers to ergocalciferol (vitamin D2), cholecalciferol (vitamin D3), and calcidiol monohydrate. Systematic reviews of the literature were conducted to assess the relative bioavailability of calcidiol monohydrate versus vitamin D3 on serum 25(OH)D concentrations, and for priority adverse health effects of excess vitamin D intake, namely persistent hypercalcaemia/hypercalciuria and endpoints related to musculoskeletal health (i.e. falls, bone fractures, bone mass/density and indices thereof). Based on the available evidence, the Panel proposes a CF for calcidiol monohydrates of 2.5 for labelling purposes. Persistent hypercalciuria, which may be an earlier sign of excess vitamin D than persistent hypercalcaemia, is selected as the critical endpoint on which to base the UL for vitamin D. A lowest-observed-adverse-effect-level (LOAEL) of 250 μg/day is identified from two randomised controlled trials in humans, to which an uncertainty factor of 2.5 is applied to account for the absence of a no-observed-adverse-effect-level (NOAEL). A UL of 100 μg vitamin D equivalents (VDE)/day is established for adults (including pregnant and lactating women) and for adolescents aged 11-17 years, as there is no reason to believe that adolescents in the phase of rapid bone formation and growth have a lower tolerance for vitamin D compared to adults. For children aged 1-10 years, a UL of 50 μg VDE/day is established by considering their smaller body size. Based on available intake data, European populations are unlikely to exceed the UL, except for regular users of food supplements containing high doses of vitamin D.
Keywords: Ergocalciferol; calcidiol monohydrate; cholecalciferol; conversion factor; tolerable upper intake level.
© 2023 European Food Safety Authority. EFSA Journal published by Wiley‐VCH GmbH on behalf of European Food Safety Authority.
Figures
References
-
- Ahn J, Yu K, Stolzenberg‐Solomon R, Simon KC, McCullough ML, Gallicchio L, Jacobs EJ, Ascherio A, Helzlsouer K, Jacobs KB, Li Q, Weinstein SJ, Purdue M, Virtamo J, Horst R, Wheeler W, Chanock S, Hunter DJ, Hayes RB, Kraft P and Albanes D, 2010. Genome‐wide association study of circulating vitamin D levels. Human Molecular Genetics, 19, 2739–2745. 10.1093/hmg/ddq155 - DOI - PMC - PubMed
-
- Akaike H, 1974. A new look at the statistical model identification. IEEE Transactions on Automatic Control, 19, 716–723.
-
- Aloia JF, Dhaliwal R, Shieh A, Mikhail M, Islam S and Yeh JK, 2013. Calcium and vitamin d supplementation in postmenopausal women. Journal of Clinical Endocrinology and Metabolism, 98, E1702–E1709. - PubMed
LinkOut - more resources
Full Text Sources