

Pertuzumab Plus Trastuzumab With or Without Chemotherapy Followed by Emtansine in ERBB2-Positive Metastatic Breast Cancer: A Secondary Analysis of a Randomized Clinical Trial
- PMID: 37561451
- PMCID: PMC10416088
- DOI: 10.1001/jamaoncol.2023.2909
Pertuzumab Plus Trastuzumab With or Without Chemotherapy Followed by Emtansine in ERBB2-Positive Metastatic Breast Cancer: A Secondary Analysis of a Randomized Clinical Trial
Abstract
Importance: In ERBB2 (formerly HER2)-positive metastatic breast cancer (MBC), combining trastuzumab and pertuzumab with taxane-based chemotherapy is the first line of standard care. Given that trastuzumab plus pertuzumab was proven effective in ERBB2-positive MBC, even without chemotherapy, whether the optimal first-line strategy could be trastuzumab plus pertuzumab alone instead of with chemotherapy is unresolved.
Objective: To assess overall survival (OS) at 2 years and progression-free survival (PFS) for patients randomly assigned to receive first-line pertuzumab plus trastuzumab alone or with chemotherapy followed by trastuzumab and emtansine at progression; PFS of second-line trastuzumab and emtansine treatment following trastuzumab plus pertuzumab; and OS and PFS in the ERBB2-enriched and ERBB2-nonenriched subtypes.
Design, setting, and participants: This was a secondary analysis of a multicenter, open-label, phase 2 randomized clinical trial conducted at 27 sites in France, 20 sites in Switzerland, 9 sites in the Netherlands, and 1 site in Germany. Overall, 210 patients with centrally confirmed ERBB2-positive MBC were randomized between May 3, 2013, and January 4, 2016, with termination of the trial May 26, 2020. Data were analyzed from December 18, 2020, to May 10, 2022.
Interventions: Patients randomly received pertuzumab (840 mg intravenously [IV], then 420 mg IV every 3 weeks) plus trastuzumab (8 mg/kg IV, then 6 mg/kg IV every 3 weeks) without chemotherapy (group A) or pertuzumab plus trastuzumab (same doses) with either paclitaxel (90 mg/m2 for days 1, 8, and 15, then every 4 weeks for ≥4 months) or vinorelbine tartrate (25 mg/m2 for first administration followed by 30 mg/m2 on days 1 and 8 and every 3 weeks for ≥4 months) followed by pertuzumab plus trastuzumab maintenance after chemotherapy discontinuation (group B).
Main outcomes and measures: Overall survival at 24 months by treatment group, PFS for first-line treatment, PFS for second-line treatment, and patient-reported quality of life (QOL).
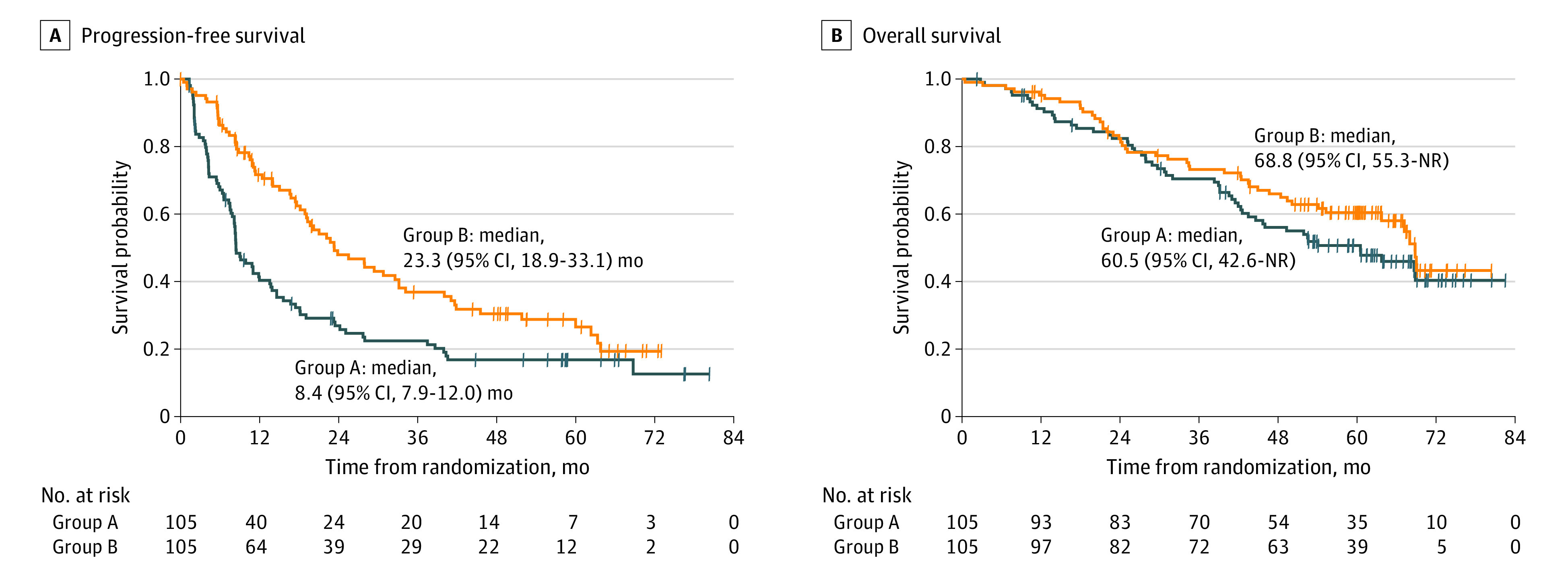
Results: A total of 210 patients were included in the analysis, with a median age of 58 (range, 26-85) years. For group A, 24-month OS was 79.0% (90% CI, 71.4%-85.4%); for group B, 78.1% (90% CI, 70.4%-84.5%). Median PFS with first-line treatment was 8.4 (95% CI, 7.9-12.0) months in group A and 23.3 (95% CI, 18.9-33.1) months in group B. Unlike expectations, OS and PFS did not markedly differ between populations with ERBB2-enriched and ERBB2-nonenriched cancer. Adverse events were less common without chemotherapy, with small QOL improvements from baseline in group A and stable QOL in group B.
Conclusions and relevance: The findings of this secondary analysis of a randomized clinical trial suggest that the chemotherapy-free anti-ERBB2 strategy is feasible without being detrimental in terms of OS. The 50-gene prediction analysis of microarray signature could not help to identify the most appropriate patient population for this approach.
Trial registration: ClinicalTrials.gov Identifier: NCT01835236.
Conflict of interest statement
Figures



Comment in
-
Is Pertuzumab Plus Trastuzumab Without Chemotherapy a Reasonable Treatment for ERBB2-Positive Metastatic Breast Cancer?JAMA Oncol. 2024 Apr 1;10(4):537. doi: 10.1001/jamaoncol.2023.6957. JAMA Oncol. 2024. PMID: 38329744 No abstract available.
References
-
- Ghislain I, Zikos E, Coens C, et al. ; European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life Group; Breast Cancer Group; EORTC Headquarters . Health-related quality of life in locally advanced and metastatic breast cancer: methodological and clinical issues in randomised controlled trials. Lancet Oncol. 2016;17(7):e294-e304. doi:10.1016/S1470-2045(16)30099-7 - DOI - PubMed
-
- Baselga J, Gelmon KA, Verma S, et al. . Phase II trial of pertuzumab and trastuzumab in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer that progressed during prior trastuzumab therapy. J Clin Oncol. 2010;28(7):1138-1144. doi:10.1200/JCO.2009.24.2024 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
