A phase III randomized crossover trial of plerixafor versus G-CSF for treatment of WHIM syndrome
- PMID: 37561579
- PMCID: PMC10541188
- DOI: 10.1172/JCI164918
A phase III randomized crossover trial of plerixafor versus G-CSF for treatment of WHIM syndrome
Abstract
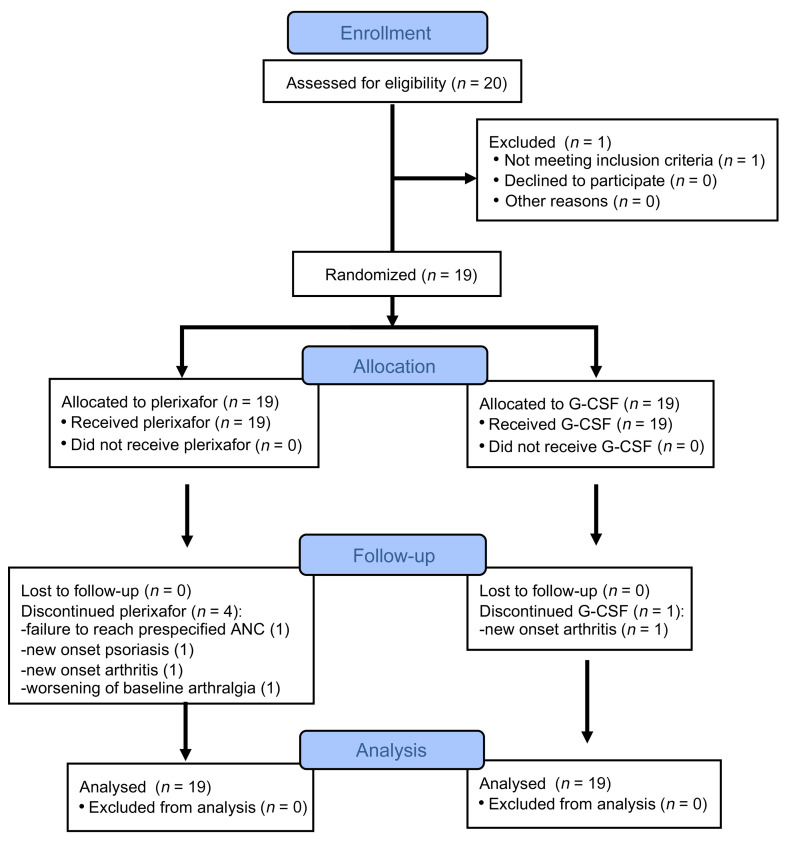
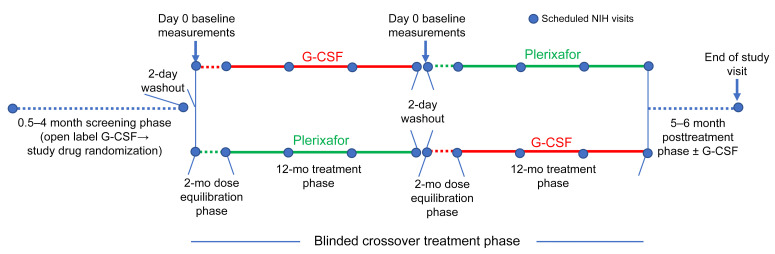
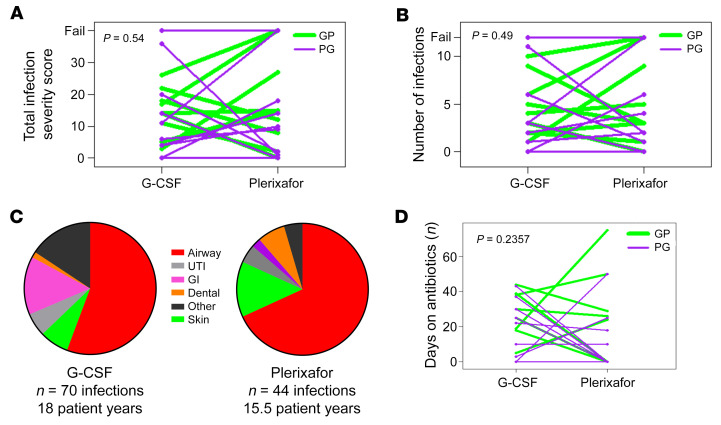
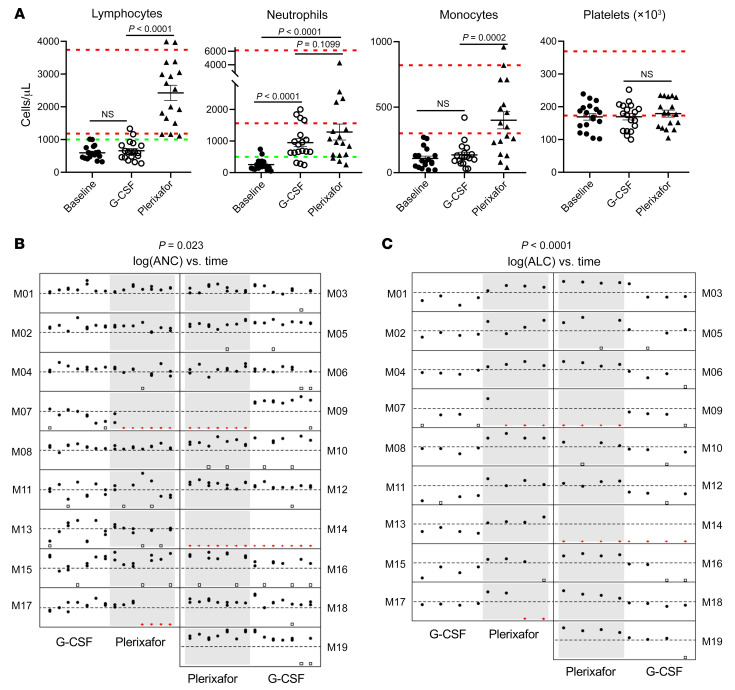
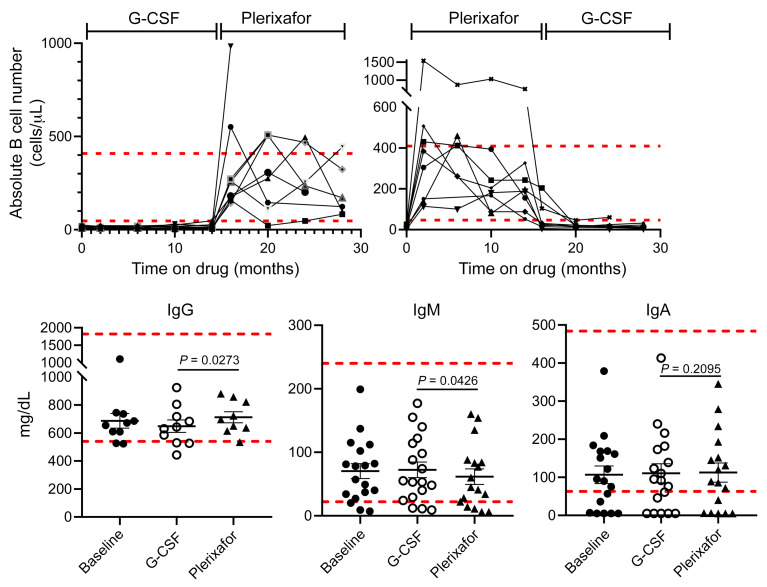
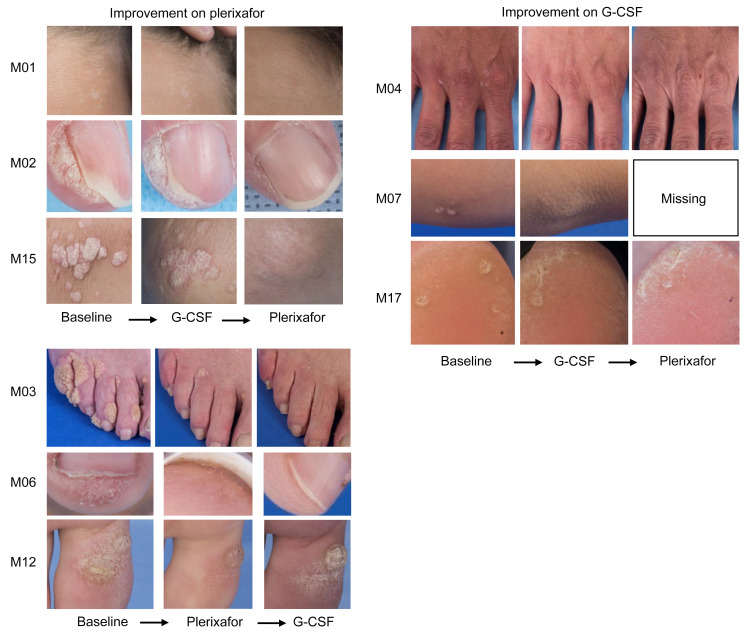
BACKGROUNDWarts, hypogammaglobulinemia, infections, and myelokathexis (WHIM) syndrome is a primary immunodeficiency disorder caused by heterozygous gain-of-function CXCR4 mutations. Myelokathexis is a kind of neutropenia caused by neutrophil retention in bone marrow and in WHIM syndrome is associated with lymphopenia and monocytopenia. The CXCR4 antagonist plerixafor mobilizes leukocytes to the blood; however, its safety and efficacy in WHIM syndrome are undefined.METHODSIn this investigator-initiated, single-center, quadruple-masked phase III crossover trial, we compared the total infection severity score (TISS) as the primary endpoint in an intent-to-treat manner in 19 patients with WHIM who each received 12 months treatment with plerixafor and 12 months treatment with granulocyte CSF (G-CSF, the standard of care for severe congenital neutropenia). The treatment order was randomized for each patient.RESULTSPlerixafor was nonsuperior to G-CSF for TISS (P = 0.54). In exploratory endpoints, plerixafor was noninferior to G-CSF for maintaining neutrophil counts of more than 500 cells/μL (P = 0.023) and was superior to G-CSF for maintaining lymphocyte counts above 1,000 cells/μL (P < 0.0001). Complete regression of a subset of large wart areas occurred on plerixafor in 5 of 7 patients with major wart burdens at baseline. Transient rash occurred on plerixafor, and bone pain was more common on G-CSF. There were no significant differences in drug preference or quality of life or the incidence of drug failure or serious adverse events.CONCLUSIONPlerixafor was not superior to G-CSF in patients with WHIM for TISS, the primary endpoint. Together with wart regression and hematologic improvement, the infection severity results support continued study of plerixafor as a potential treatment for WHIM syndrome.TRIAL REGISTRATIONClinicaltrials.gov NCT02231879.FUNDINGThis study was funded by the Division of Intramural Research, National Institute of Allergy and Infectious Diseases.
Keywords: Clinical Trials; Genetic diseases; Immunology; Innate immunity; Neutrophils.
Figures