

Delineation and agreement of FET PET biological volumes in glioblastoma: results of the nuclear medicine credentialing program from the prospective, multi-centre trial evaluating FET PET In Glioblastoma (FIG) study-TROG 18.06
- PMID: 37563351
- PMCID: PMC10611835
- DOI: 10.1007/s00259-023-06371-5
Delineation and agreement of FET PET biological volumes in glioblastoma: results of the nuclear medicine credentialing program from the prospective, multi-centre trial evaluating FET PET In Glioblastoma (FIG) study-TROG 18.06
Abstract
Purpose: The O-(2-[18F]-fluoroethyl)-L-tyrosine (FET) PET in Glioblastoma (FIG) trial is an Australian prospective, multi-centre study evaluating FET PET for glioblastoma patient management. FET PET imaging timepoints are pre-chemoradiotherapy (FET1), 1-month post-chemoradiotherapy (FET2), and at suspected progression (FET3). Before participant recruitment, site nuclear medicine physicians (NMPs) underwent credentialing of FET PET delineation and image interpretation.
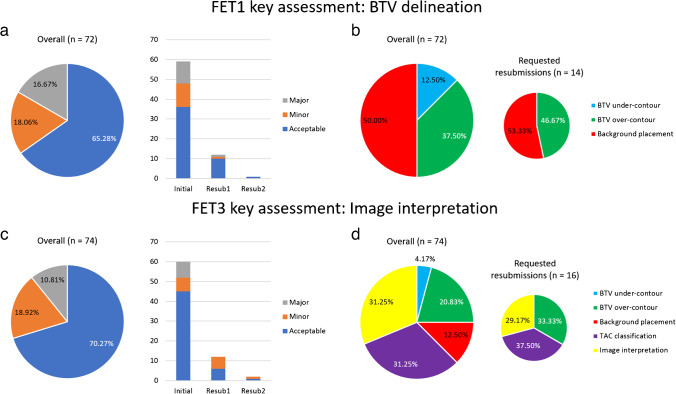
Methods: Sites were required to complete contouring and dynamic analysis by ≥ 2 NMPs on benchmarking cases (n = 6) assessing biological tumour volume (BTV) delineation (3 × FET1) and image interpretation (3 × FET3). Data was reviewed by experts and violations noted. BTV definition includes tumour-to-background ratio (TBR) threshold of 1.6 with crescent-shaped background contour in the contralateral normal brain. Recurrence/pseudoprogression interpretation (FET3) required assessment of maximum TBR (TBRmax), dynamic analysis (time activity curve [TAC] type, time to peak), and qualitative assessment. Intraclass correlation coefficient (ICC) assessed volume agreement, coefficient of variation (CoV) compared maximum/mean TBR (TBRmax/TBRmean) across cases, and pairwise analysis assessed spatial (Dice similarity coefficient [DSC]) and boundary agreement (Hausdorff distance [HD], mean absolute surface distance [MASD]).
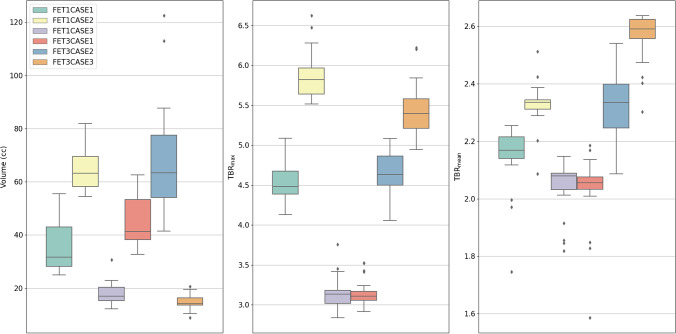
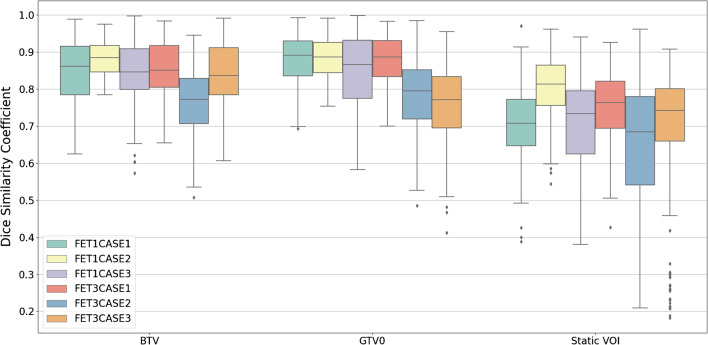
Results: Data was accrued from 21 NMPs (10 centres, n ≥ 2 each) and 20 underwent review. The initial pass rate was 93/119 (78.2%) and 27/30 requested resubmissions were completed. Violations were found in 25/72 (34.7%; 13/12 minor/major) of FET1 and 22/74 (29.7%; 14/8 minor/major) of FET3 reports. The primary reasons for resubmission were as follows: BTV over-contour (15/30, 50.0%), background placement (8/30, 26.7%), TAC classification (9/30, 30.0%), and image interpretation (7/30, 23.3%). CoV median and range for BTV, TBRmax, and TBRmean were 21.53% (12.00-30.10%), 5.89% (5.01-6.68%), and 5.01% (3.37-6.34%), respectively. BTV agreement was moderate to excellent (ICC = 0.82; 95% CI, 0.63-0.97) with good spatial (DSC = 0.84 ± 0.09) and boundary (HD = 15.78 ± 8.30 mm; MASD = 1.47 ± 1.36 mm) agreement.
Conclusion: The FIG study credentialing program has increased expertise across study sites. TBRmax and TBRmean were robust, with considerable variability in BTV delineation and image interpretation observed.
Keywords: Clinical trials; Credentialing; FET PET; Glioblastoma; Inter-observer.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Boosting the acceptance of 18F-FET PET for image-guided treatment planning with a multi-centric prospective trial.Eur J Nucl Med Mol Imaging. 2023 Nov;50(13):3817-3819. doi: 10.1007/s00259-023-06426-7. Eur J Nucl Med Mol Imaging. 2023. PMID: 37682302 Free PMC article. No abstract available.
References
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJB, Janzer RC, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. doi: 10.1016/s1470-2045(09)70025-7. - DOI - PubMed
-
- Albert NL, Weller M, Suchorska B, Galldiks N, Soffietti R, Kim MM, et al. Response Assessment in Neuro-Oncology working group and European Association for Neuro-Oncology recommendations for the clinical use of PET imaging in gliomas. Neuro Oncol. 2016;18:1199–1208. doi: 10.1093/neuonc/now058. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
