

Prognostic Nutritional Index (PNI) as a potential predictor and intervention target for perioperative ischemic stroke: a retrospective cohort study
- PMID: 37563630
- PMCID: PMC10413636
- DOI: 10.1186/s12871-023-02216-8
Prognostic Nutritional Index (PNI) as a potential predictor and intervention target for perioperative ischemic stroke: a retrospective cohort study
Abstract
Background: The prognostic nutritional index (PNI) is a nutritional indicator and predictor of various diseases. However it is unclear whether PNI can be a predictor of perioperative ischemic stroke. This study aims to evaluate the association of the preoperative PNI and ischemic stroke in patients undergoing non-cardiac surgery.
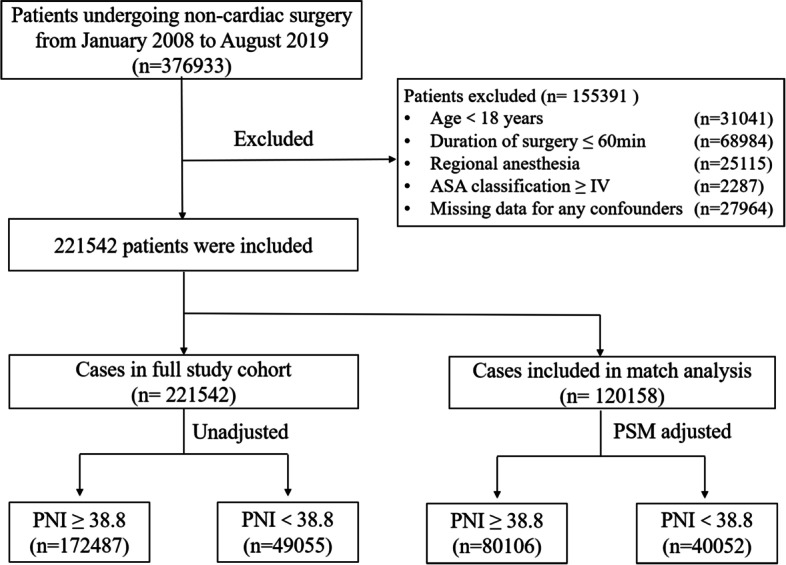
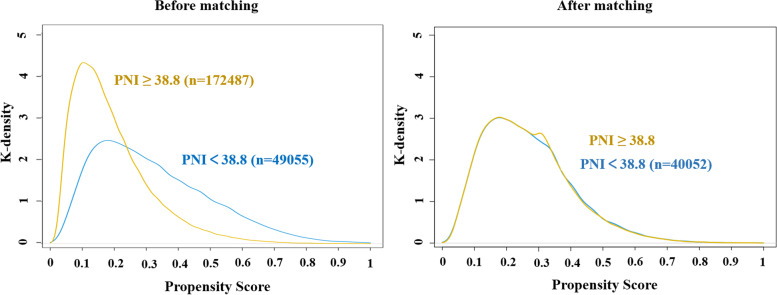
Methods: The retrospective cohort study included patients who underwent noncardiac surgery between January 2008 and August 2019. The patients were divided into PNI ≥ 38.8 and PNI < 38.8 groups according to the cut-off value of PNI. Univariate and multivariate logistic regression analyses were performed to explore the association between PNI and perioperative ischemic stroke. Subsequently, propensity score matching (PSM) analysis was performed to eliminate the confounding factors of covariates and further validate the results. Subgroup analyses were completed to assess the predictive utility of PNI for perioperative ischemic stroke in different groups.
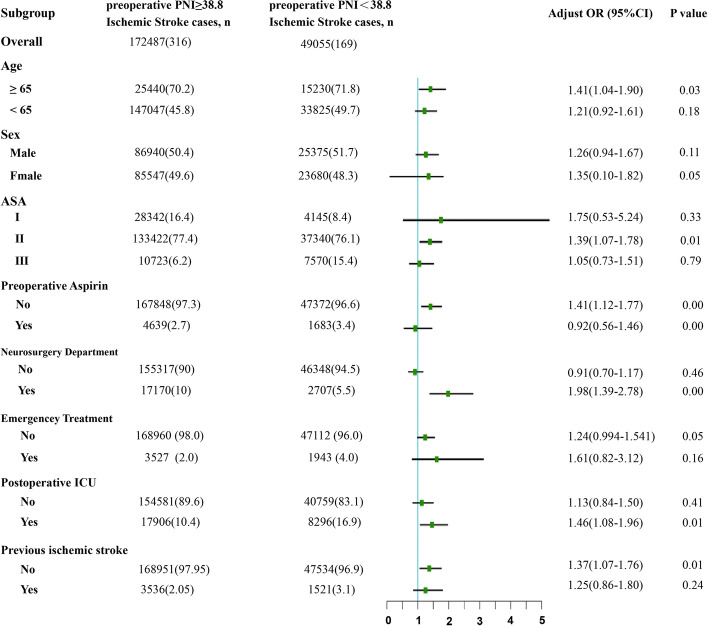
Results: Amongst 221,542 hospitalized patients enrolled, 485 (0.22%) experienced an ischemic stroke within 30 days of the surgery, 22.1% of patients were malnourished according to PNI < 38.8, and the occurrence of perioperative ischemic stroke was 0.34% (169/49055) in the PNI < 38.8 group. PNI < 38.8 was significantly associated with an increased incidence of perioperative ischemic stroke whether in univariate logistic regression analysis (OR = 1.884, 95% CI: 1.559-2.267, P < 0.001) or multivariate logistic regression analysis (OR = 1.306, 95% CI: 1.061-1.602, P = 0.011). After PSM analysis, the ORs of PNI < 38.8 group were 1.250 (95% CI: 1.000-1.556, P = 0.050) and 1.357 (95% CI: 1.077-1.704, P = 0.009) in univariate logistic regression analysis and multivariate logistic regression analysis respectively. The subgroup analysis indicated that reduced PNI was significantly associated to an increased risk of perioperative ischemic stroke in patients over 65 years old, ASA II, not taking aspirin before surgery, without a history of stroke, who had neurosurgery, non-emergency surgery, and were admitted to ICU after surgery.
Conclusions: Our study indicates that low preoperative PNI is significantly associated with a higher incidence of ischemic stroke in patients undergoing non-cardiac surgery. Preoperative PNI, as a preoperative nutritional status evaluation index, is an independent risk factor useful to predict perioperative ischemic stroke risk, which could be used as an intervenable preoperative clinical biochemical index to reduce the incidence of perioperative ischemic stroke.
Keywords: Intervention target; Perioperative ischemic stroke; Postoperative complication; Predictor; Prognostic Nutritional Index (PNI).
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Elevated risk of perioperative ischemic stroke in noncardiac surgery patients with atrial fibrillation: a retrospective cohort study.BMC Anesthesiol. 2025 Apr 2;25(1):151. doi: 10.1186/s12871-025-03011-3. BMC Anesthesiol. 2025. PMID: 40175937 Free PMC article.
-
Preoperative prognostic nutritional index predicts postoperative delirium in aged patients after surgery: A matched cohort study.Gen Hosp Psychiatry. 2024 Jan-Feb;86:58-66. doi: 10.1016/j.genhosppsych.2023.11.013. Epub 2023 Dec 5. Gen Hosp Psychiatry. 2024. PMID: 38101151
-
Systemic-Immune-Inflammation Index as a Promising Biomarker for Predicting Perioperative Ischemic Stroke in Older Patients Who Underwent Non-cardiac Surgery.Front Aging Neurosci. 2022 Apr 1;14:865244. doi: 10.3389/fnagi.2022.865244. eCollection 2022. Front Aging Neurosci. 2022. PMID: 35431888 Free PMC article.
-
Prognostic nutritional index as a predictor of mortality in acute ischemic stroke.Clin Neurol Neurosurg. 2025 Feb;249:108750. doi: 10.1016/j.clineuro.2025.108750. Epub 2025 Jan 17. Clin Neurol Neurosurg. 2025. PMID: 39847887
-
Prognostic Nutritional Index and the Risk of Postoperative Complications After Spine Surgery: A Meta-Analysis.World Neurosurg. 2024 May;185:e572-e581. doi: 10.1016/j.wneu.2024.02.077. Epub 2024 Feb 19. World Neurosurg. 2024. PMID: 38382761
Cited by
-
The role of the prognostic nutritional index in predicting mortality in stroke patients.Rev Assoc Med Bras (1992). 2024 Sep 13;70(9):e20240714. doi: 10.1590/1806-9282.20240714. eCollection 2024. Rev Assoc Med Bras (1992). 2024. PMID: 39292077 Free PMC article.
-
Higher Neutrophil-to-Lymphocyte Ratio and Systemic Immune-Inflammation Index Is Associated with Better Prognosis Following Pancreaticoduodenectomy for Pancreatic Adenocarcinoma.J Clin Med. 2025 May 27;14(11):3762. doi: 10.3390/jcm14113762. J Clin Med. 2025. PMID: 40507524 Free PMC article.
-
Construction of a predictive model for concurrent infection in liver failure patients based on prognostic nutritional index and inflammatory cytokine analysis.BMC Gastroenterol. 2025 Aug 19;25(1):598. doi: 10.1186/s12876-025-04054-z. BMC Gastroenterol. 2025. PMID: 40830428 Free PMC article.
-
A Diagnostic Nomogram Incorporating Prognostic Nutritional Index for Predicting Vaginal Invasion in Stage IB - IIA Cervical Cancer.Cancer Control. 2024 Jan-Dec;31:10732748241278479. doi: 10.1177/10732748241278479. Cancer Control. 2024. PMID: 39171582 Free PMC article.
-
The Correlation and Predictive Value of Prognostic Nutrition Index with Vasovagal Syncope in Children.Pediatr Cardiol. 2025 Apr 17. doi: 10.1007/s00246-025-03863-z. Online ahead of print. Pediatr Cardiol. 2025. PMID: 40244319
References
-
- Parikh S, Cohen JR. Perioperative stroke after general surgical procedures. N Y State J Med. 1993;93(3):162–165. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
