

Predicting response to immunotherapy in gastric cancer via assessing perineural invasion-mediated inflammation in tumor microenvironment
- PMID: 37563649
- PMCID: PMC10416472
- DOI: 10.1186/s13046-023-02730-0
Predicting response to immunotherapy in gastric cancer via assessing perineural invasion-mediated inflammation in tumor microenvironment
Abstract
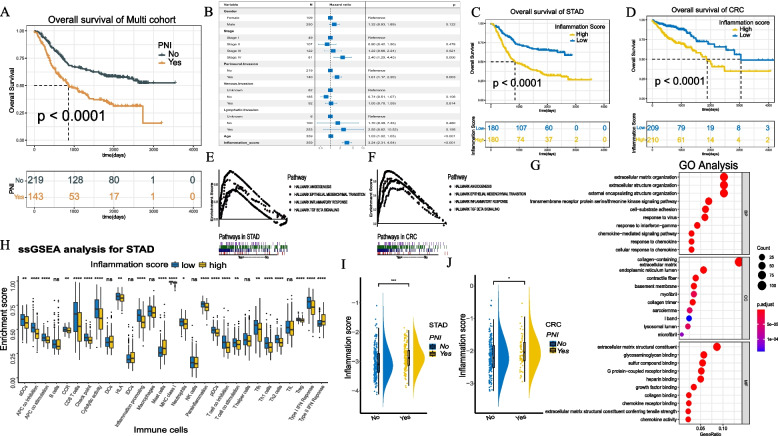
Background: The perineural invasion (PNI)-mediated inflammation of the tumor microenvironment (TME) varies among gastric cancer (GC) patients and exhibits a close relationship with prognosis and immunotherapy. Assessing the neuroinflammation of TME is important in predicting the response to immunotherapy in GC patients.
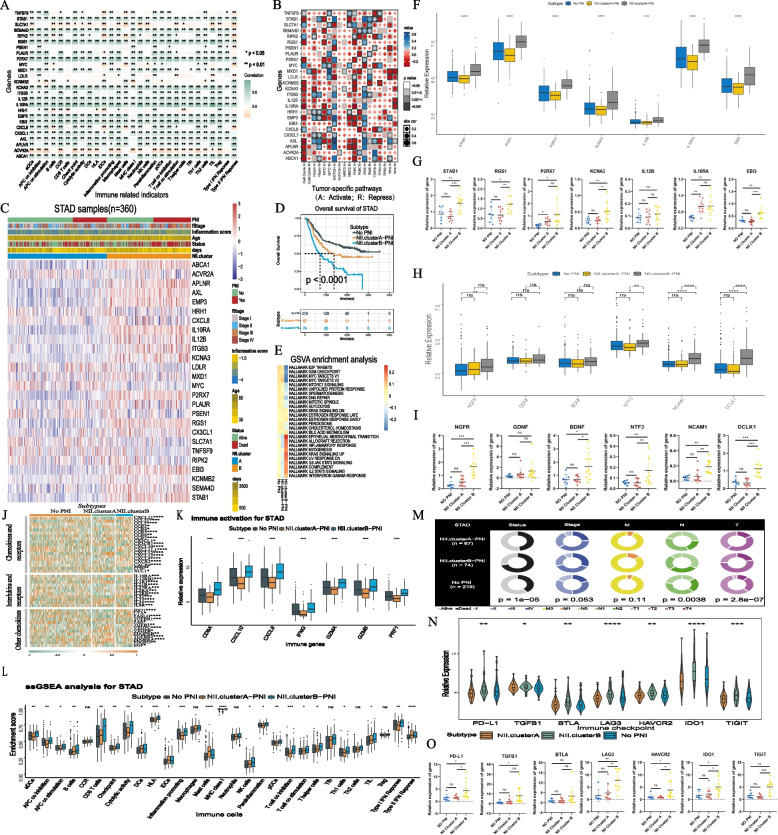
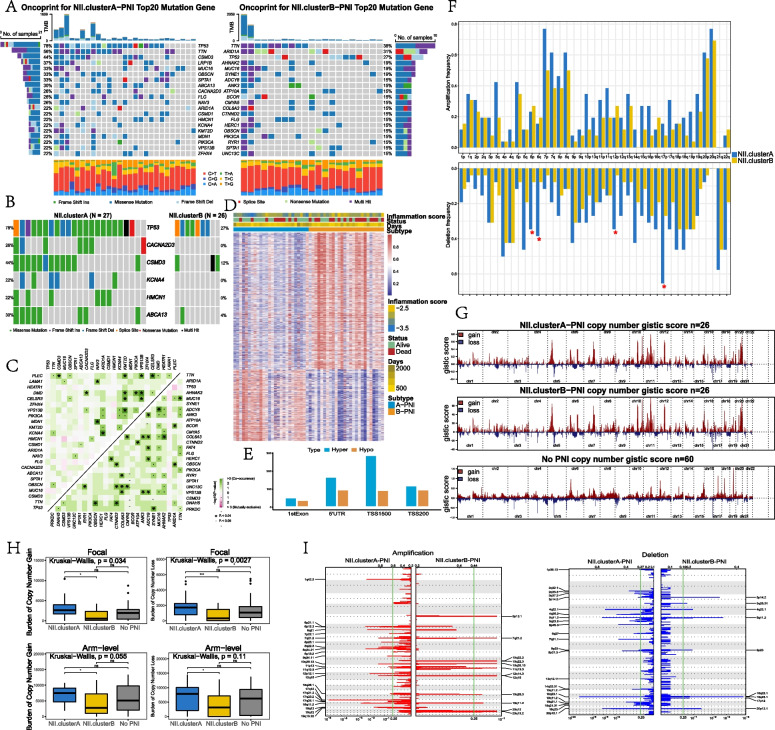
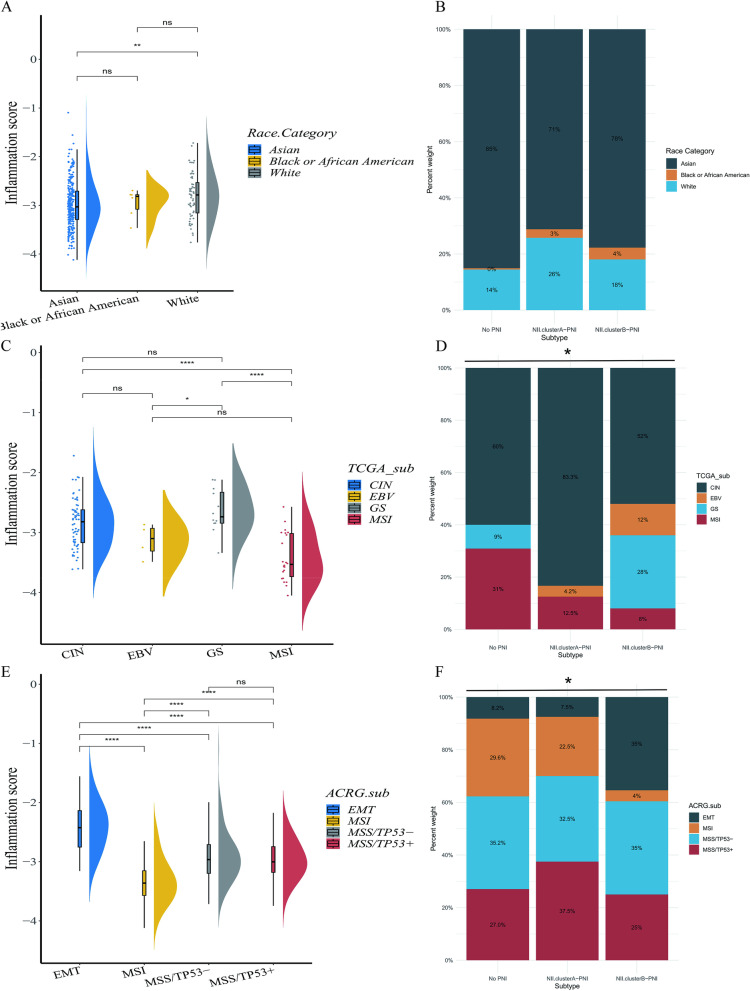
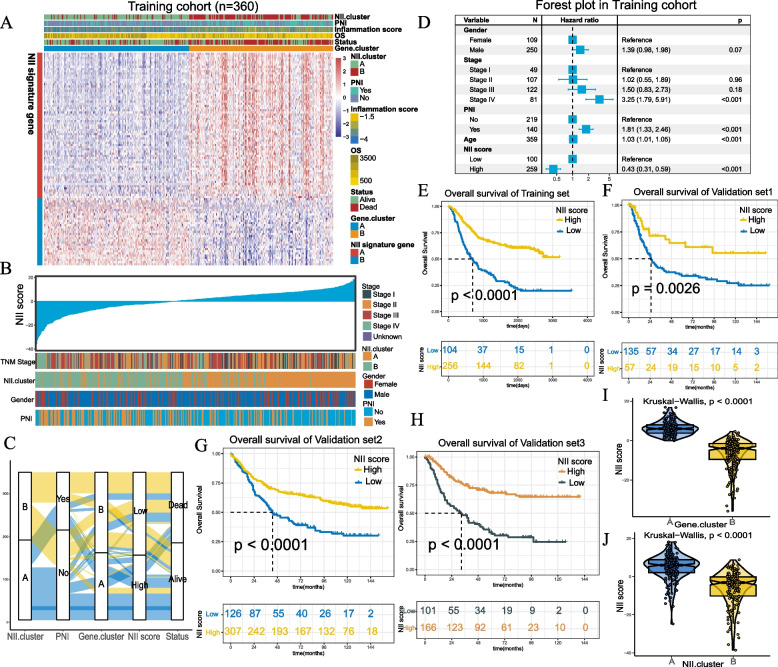
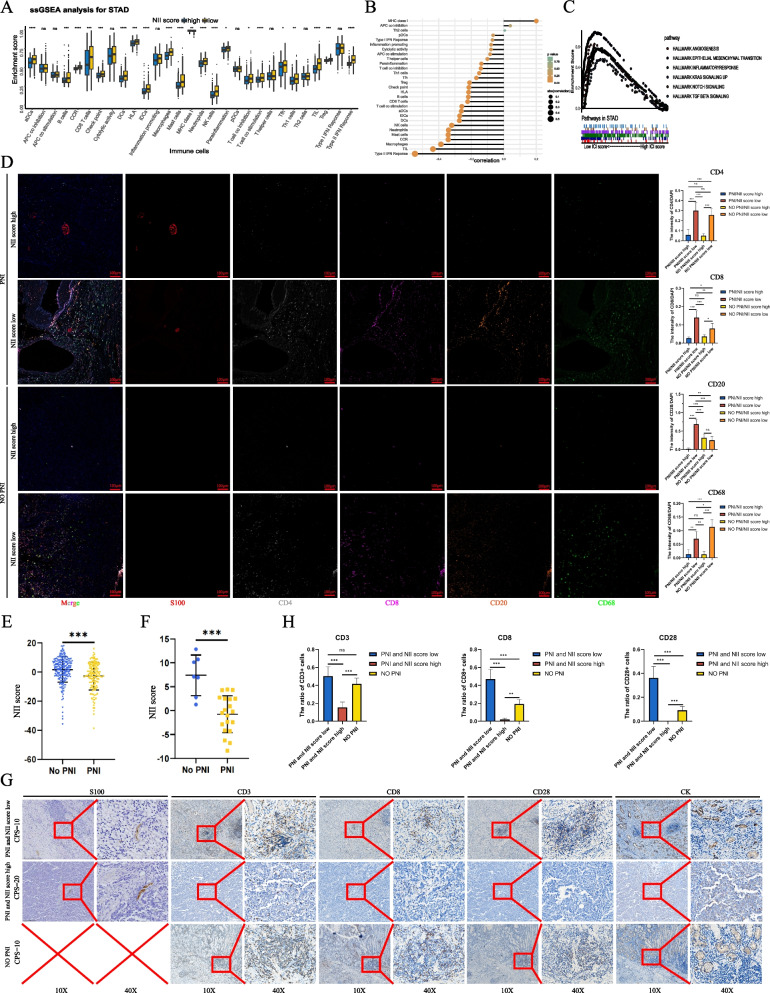
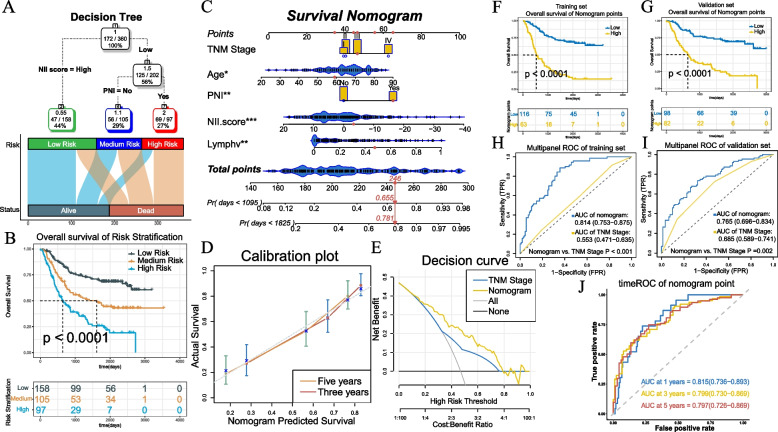
Methods: Fifteen independent cohorts were enrolled in this study. An inflammatory score was developed and validated in GC. Based on PNI-related prognostic inflammatory signatures, patients were divided into Clusters A and B using unsupervised clustering. The characteristics of clusters and the potential regulatory mechanism of key genes were verified by RT-PCR, western-blot, immunohistochemistry and immunofluorescence in cell and tumor tissue samples.The neuroinflammation infiltration (NII) scoring system was developed based on principal component analysis (PCA) and visualized in a nomogram together with other clinical characteristics.
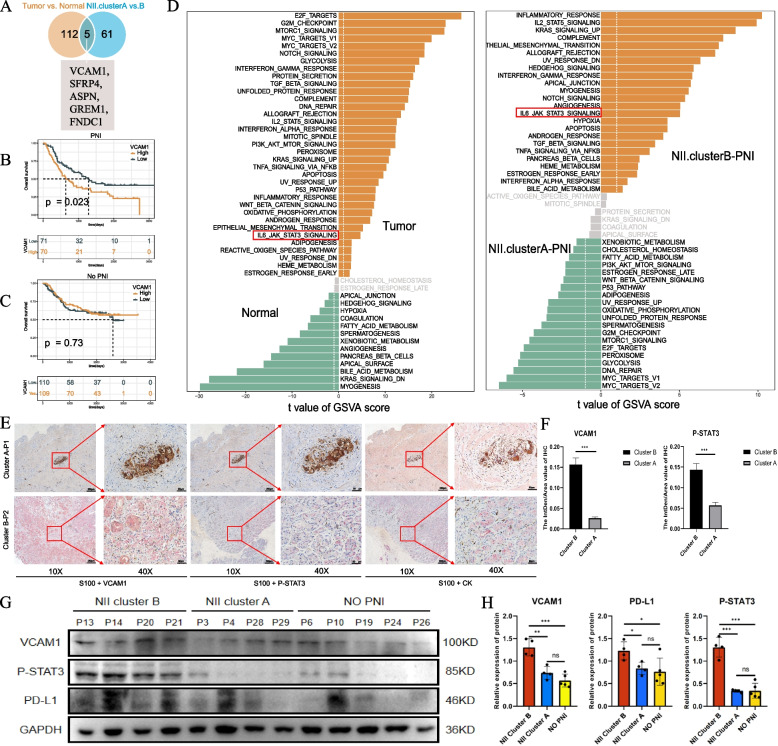
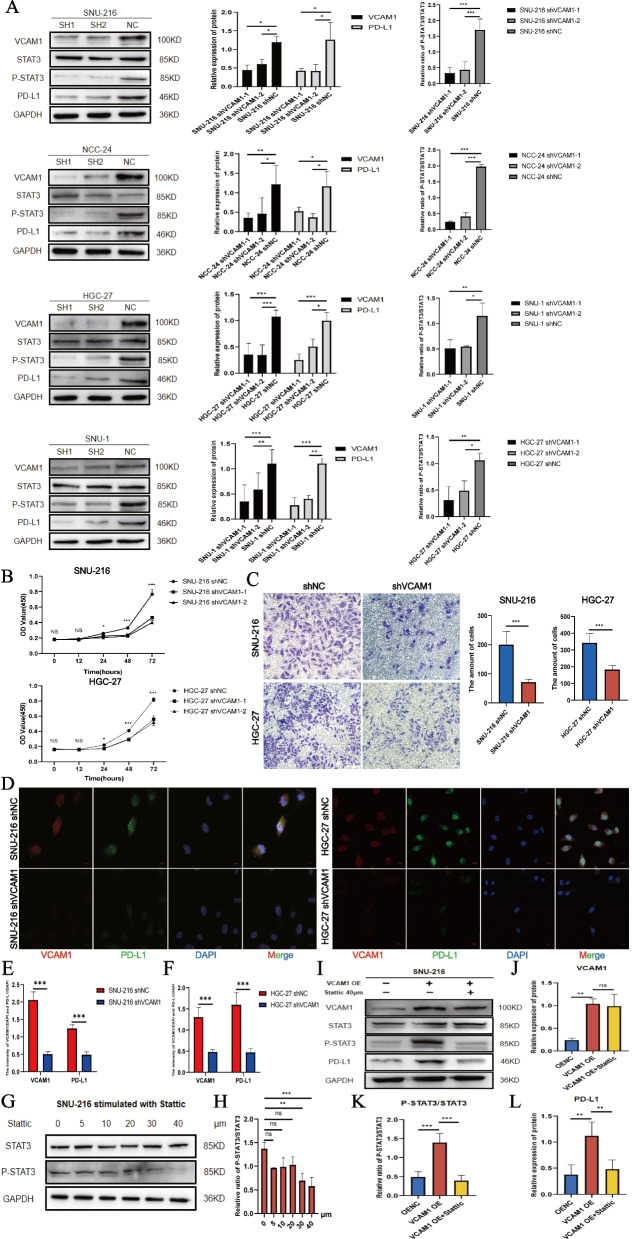
Results: Inflammatory scores were higher in GC patients with PNI compared with those without PNI (P < 0.001). NII.clusterB patients with PNI had abundant immune cell infiltration in the TME but worse prognosis compared with patients in the NII.clusterA patients with PNI and non-PNI subgroups. Higher immune checkpoint expression was noted in NII.clusterB-PNI. VCAM1 is a specific signature of NII.clusterB-PNI, which regulates PD-L1 expression by affecting the phosphorylation of STAT3 in GC cells. Patients with PNI and high NII scores may benefit from immunotherapy. Patients with low nomogram scores had a better prognosis than those with high nomogram scores.
Conclusions: Inflammation mediated by PNI is one of the results of tumor-nerve crosstalk, but its impact on the tumor immune microenvironment is complex. Assessing the inflammation features of PNI is a potential method in predicting the response of immunotherapy effectively.
Keywords: Gastric cancer(GC); Inflammatory; Neuroinflammation infiltration(NII) score system; Perinueral invasion(PNI); Tumor microenvironment(TME).
© 2023. Italian National Cancer Institute ‘Regina Elena’.
Conflict of interest statement
The authors declare no conficts of interest.
Figures
References
-
- Bapat AA, et al. Perineural invasion and associated pain in pancreatic cancer. Nat Rev Cancer. 2011;11(10):695–707. - PubMed
-
- Wang K, et al. Nervous system and gastric cancer. Biochim Biophys Acta Rev Cancer. 2020;1873(1):188313. - PubMed
-
- Lubig S, et al. Quantitative perineural invasion is a prognostic marker in prostate cancer. Pathology. 2018;50(3):298–304. - PubMed
-
- Batsakis JG. Nerves and neurotropic carcinomas. Ann Otol Rhinol Laryngol. 1985;94(4 Pt 1):426–427. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
