

Real-world evidence on the dosing and safety of C.E.R.A. in pediatric dialysis patients: findings from the International Pediatric Dialysis Network registries
- PMID: 37566114
- PMCID: PMC10817843
- DOI: 10.1007/s00467-023-05977-z
Real-world evidence on the dosing and safety of C.E.R.A. in pediatric dialysis patients: findings from the International Pediatric Dialysis Network registries
Abstract
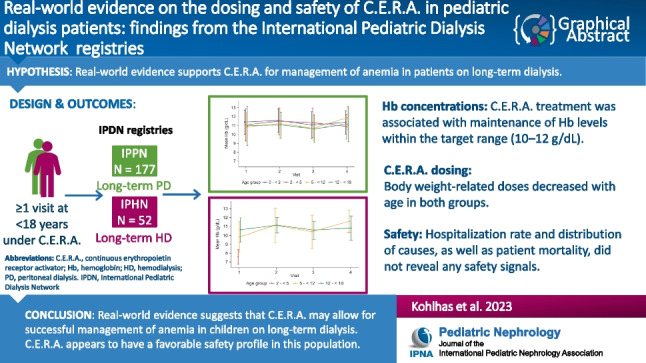
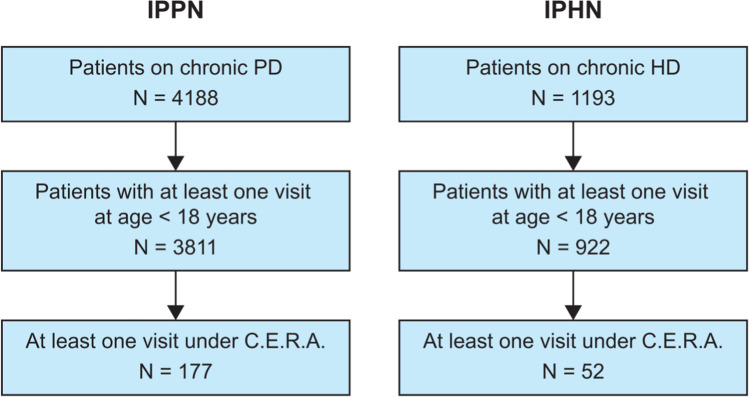
Background: This retrospective real-world study used data from two registries, International Pediatric Peritoneal Dialysis Network (IPPN) and International Pediatric Hemodialysis Network (IPHN), to characterize the efficacy and safety of continuous erythropoietin receptor activator (C.E.R.A.) in pediatric patients with chronic kidney disease (CKD) on peritoneal dialysis (PD) or hemodialysis (HD).
Methods: IPPN and IPHN collect prospective data (baseline and every 6 months) from pediatric PD and HD centers worldwide. Demographics, clinical characteristics, dialysis information, treatment, laboratory parameters, number and causes of hospitalization events, and deaths were extracted for patients on C.E.R.A. treatment (IPPN: 2007-2021; IPHN: 2013-2021).
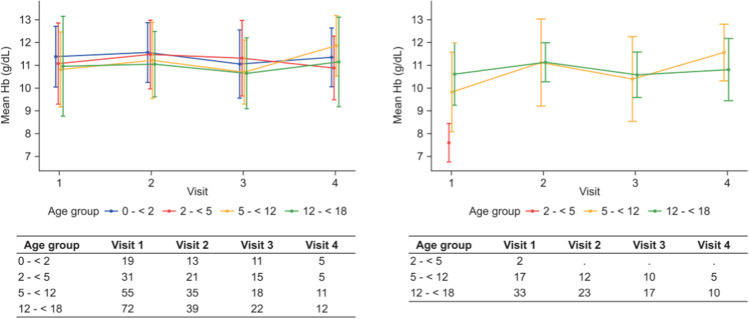
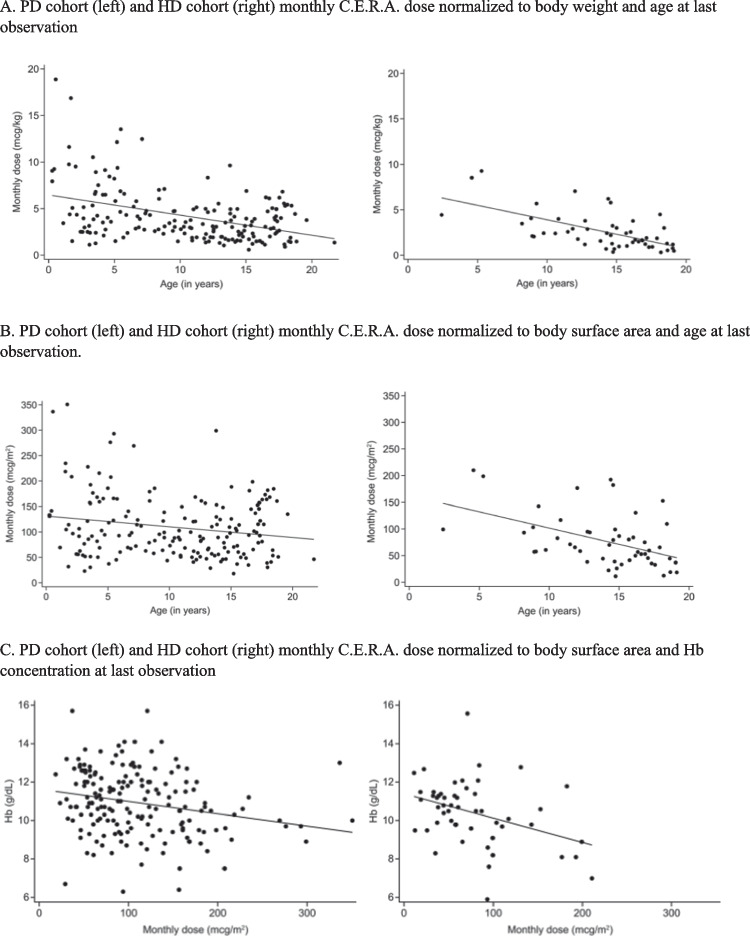
Results: We analyzed 177 patients on PD (median age 10.6 years) and 52 patients on HD (median age 14.1 years) who had ≥ 1 observation while being treated with C.E.R.A. The median (interquartile range [IQR]) observation time under C.E.R.A. exposure was 6 (0-12.5) and 12 (0-18) months, respectively. Hemoglobin concentrations were stable over time; respective means (standard deviation) at last observation were 10.9 (1.7) g/dL and 10.4 (1.7) g/dL. Respective median (IQR) monthly C.E.R.A. doses at last observation were 3.5 (2.3-5.1) µg/kg, or 95 (62-145) µg/m2 and 2.1 (1.2-3.4) µg/kg, or 63 (40-98) µg/m2. Non-elective hospitalizations occurred in 102 (58%) PD and 32 (62%) HD patients. Seven deaths occurred (19.8 deaths per 1000 observation years).
Conclusions: C.E.R.A. was associated with efficient maintenance of hemoglobin concentrations in pediatric patients with CKD on dialysis, and appeared to have a favorable safety profile. The current analysis revealed no safety signals.
Keywords: Chronic kidney disease; Continuous erythropoietin receptor activator; Hemodialysis; Peritoneal dialysis; Real-world study.
© 2023. The Author(s).
Conflict of interest statement
Laura Kohlhas reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Milena Studer is an employee of F. Hoffmann-La Roche and reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Loes Rutten-Jacobs is an employee of F. Hoffmann-La Roche Ltd. and owns stock in F. Hoffmann-La Roche and reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Sylvie Meyer Reigner is an employee of F. Hoffmann-La Roche Ltd and reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Anja Sander reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Hui-Kim Yap reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Karel Vondrak reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Paula A. Coccia reports consulting fees, lectures and speakers’ bureaus with Fresenius medical care and Alexion, and reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Francisco Cano reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Claus Peter Schmitt received consultancy honoraria from Baxter, Iperboreal Pharma, STADAPHARM, and lecturing honoraria from Fresenius and reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Bradley A. Warady reports paid consultancy activities for Amgen, Fibrogen, Roche, Bayer, and Reata and reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Franz Schaefer reports paid consultancy activities for Amgen, Akebia, Astellas, and Roche, and reports research funding for support for third-party writing assistance from F. Hoffmann-La Roche Ltd.
Figures
Similar articles
-
Subcutaneous C.E.R.A. for the Maintenance Treatment of Anemia in Pediatric Patients With CKD: A Phase 2, Open-Label, Single-Arm, Multicenter Study.Am J Kidney Dis. 2023 Jun;81(6):684-694.e1. doi: 10.1053/j.ajkd.2022.11.006. Epub 2022 Dec 29. Am J Kidney Dis. 2023. PMID: 36587890 Clinical Trial.
-
Efficacy and Long-Term Safety of C.E.R.A. Maintenance in Pediatric Hemodialysis Patients with Anemia of CKD.Clin J Am Soc Nephrol. 2018 Jan 6;13(1):81-90. doi: 10.2215/CJN.03570417. Epub 2017 Nov 2. Clin J Am Soc Nephrol. 2018. PMID: 29097481 Free PMC article. Clinical Trial.
-
Continuous Erythropoietin Receptor Activator for the Treatment of Chronic Dialysis Patients with Renal Anemia in Daily Clinical Practice in Poland: A Non-Interventional, Multi-Center, Pragmatic NAVIGO Trial.Nephron. 2024;148(2):104-112. doi: 10.1159/000534070. Epub 2023 Sep 14. Nephron. 2024. PMID: 37708860 Free PMC article.
-
Urgent-start peritoneal dialysis versus haemodialysis for people with chronic kidney disease.Cochrane Database Syst Rev. 2021 Jan 27;1(1):CD012899. doi: 10.1002/14651858.CD012899.pub2. Cochrane Database Syst Rev. 2021. PMID: 33501650 Free PMC article.
-
Targeting optimal PD management in children: what have we learned from the IPPN registry?Pediatr Nephrol. 2021 May;36(5):1053-1063. doi: 10.1007/s00467-020-04598-0. Epub 2020 May 27. Pediatr Nephrol. 2021. PMID: 32458134 Free PMC article. Review.
Cited by
-
Realizing the promise of real-world data in pediatric kidney disease: a work in progress.Pediatr Nephrol. 2024 Mar;39(3):641-643. doi: 10.1007/s00467-023-06202-7. Epub 2023 Nov 13. Pediatr Nephrol. 2024. PMID: 37955703 No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
