

Anesthesia Clinical Workload Estimated From Electronic Health Record Documentation vs Billed Relative Value Units
- PMID: 37566415
- PMCID: PMC10422189
- DOI: 10.1001/jamanetworkopen.2023.28514
Anesthesia Clinical Workload Estimated From Electronic Health Record Documentation vs Billed Relative Value Units
Abstract
Importance: Accurate measurements of clinical workload are needed to inform health care policy. Existing methods for measuring clinical workload rely on surveys or time-motion studies, which are labor-intensive to collect and subject to biases.
Objective: To compare anesthesia clinical workload estimated from electronic health record (EHR) audit log data vs billed relative value units.
Design, setting, and participants: This cross-sectional study of anesthetic encounters occurring between August 26, 2019, and February 9, 2020, used data from 8 academic hospitals, community hospitals, and surgical centers across Missouri and Illinois. Clinicians who provided anesthetic services for at least 1 surgical encounter were included. Data were analyzed from January 2022 to January 2023.
Exposure: Anesthetic encounters associated with a surgical procedure were included. Encounters associated with labor analgesia and endoscopy were excluded.
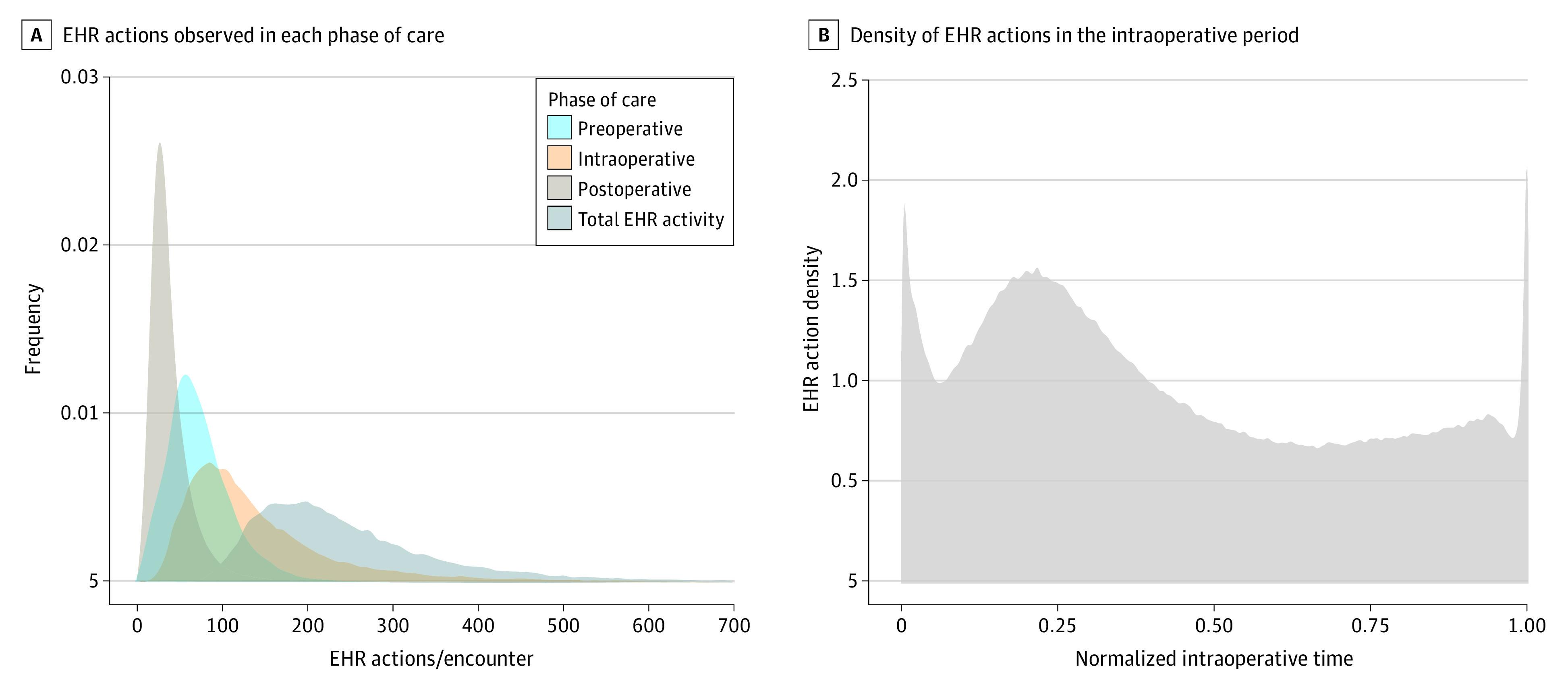
Main outcomes and measures: For each encounter, EHR-derived clinical workload was estimated as the sum of all EHR actions recorded in the audit log by anesthesia clinicians who provided care. Billing-derived clinical workload was measured as the total number of units billed for the encounter. A linear mixed-effects model was used to estimate the relative contribution of patient complexity (American Society of Anesthesiology [ASA] physical status modifier), procedure complexity (ASA base unit value for the procedure), and anesthetic duration (time units) to EHR-derived and billing-derived workload. The resulting β coefficients were interpreted as the expected effect of a 1-unit change in each independent variable on the standardized workload outcome. The analysis plan was developed after the data were obtained.
Results: A total of 405 clinicians who provided anesthesia for 31 688 encounters were included in the study. A total of 8 288 132 audit log actions corresponding to 39 131 hours of EHR use were used to measure EHR-derived workload. The contributions of patient complexity, procedural complexity, and anesthesia duration to EHR-derived workload differed significantly from their contributions to billing-derived workload. The contribution of patient complexity toward EHR-derived workload (β = 0.162; 95% CI, 0.153-0.171) was more than 50% greater than its contribution toward billing-derived workload (β = 0.106; 95% CI, 0.097-0.116; P < .001). In contrast, the contribution of procedure complexity toward EHR-derived workload (β = 0.033; 95% CI, 0.031-0.035) was approximately one-third its contribution toward billing-derived workload (β = 0.106; 95% CI, 0.104-0.108; P < .001).
Conclusions and relevance: In this cross-sectional study of 8 hospitals, reimbursement for anesthesiology services overcompensated for procedural complexity and undercompensated for patient complexity. This method for measuring clinical workload could be used to improve reimbursement valuations for anesthesia and other specialties.
Conflict of interest statement
Figures



Similar articles
-
The impact of longer-than-average anesthesia times on the billing of academic anesthesiology departments.Anesth Analg. 2001 Dec;93(6):1537-43, table of contents. doi: 10.1097/00000539-200112000-00042. Anesth Analg. 2001. PMID: 11726438
-
Industry-Wide Survey of Academic Anesthesiology Departments Provides Up-to-Date Benchmarking Data on Surgical Anesthesia Productivity.Anesth Analg. 2020 Sep;131(3):885-892. doi: 10.1213/ANE.0000000000004934. Anesth Analg. 2020. PMID: 32541253
-
A Scalable and Extensible Logical Data Model of Electronic Health Record Audit Logs for Temporal Data Mining (RNteract): Model Conceptualization and Formulation.JMIR Nurs. 2024 Jun 24;7:e55793. doi: 10.2196/55793. JMIR Nurs. 2024. PMID: 38913994 Free PMC article.
-
The challenges of implementing electronic health records for anesthesia use outside the operating room.Curr Opin Anaesthesiol. 2016 Aug;29(4):531-5. doi: 10.1097/ACO.0000000000000349. Curr Opin Anaesthesiol. 2016. PMID: 27064215 Review.
-
Future of electronic health records: implications for decision support.Mt Sinai J Med. 2012 Nov-Dec;79(6):757-68. doi: 10.1002/msj.21351. Mt Sinai J Med. 2012. PMID: 23239213 Review.
Cited by
-
Emerging Domains for Measuring Health Care Delivery With Electronic Health Record Metadata.J Med Internet Res. 2025 Mar 6;27:e64721. doi: 10.2196/64721. J Med Internet Res. 2025. PMID: 40053814 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
