

Salpingectomy and the Risk of Ovarian Cancer in Ontario
- PMID: 37566421
- PMCID: PMC10422181
- DOI: 10.1001/jamanetworkopen.2023.27198
Salpingectomy and the Risk of Ovarian Cancer in Ontario
Abstract
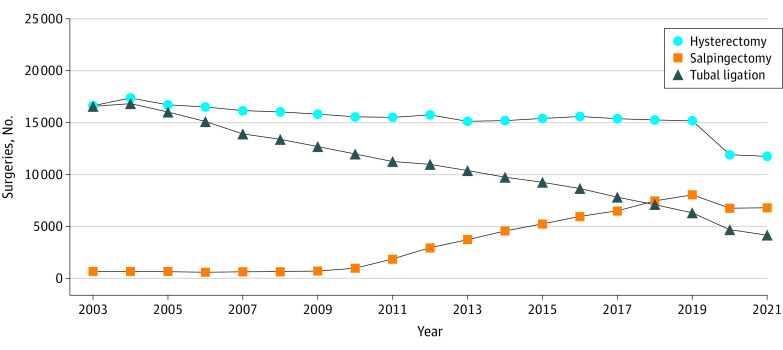
Importance: A body of pathological and clinical evidence supports the position that the fallopian tube is the site of origin for a large proportion of high-grade serous ovarian cancers. Consequently, salpingectomy is now considered for permanent contraception (in lieu of tubal ligation) or ovarian cancer prevention (performed opportunistically at the time of surgical procedures for benign gynecologic conditions).
Objective: To evaluate the association between salpingectomy and the risk of invasive epithelial ovarian, fallopian tube, and peritoneal cancer.
Design, setting, and participants: This population-based retrospective cohort study included all women aged 18 to 80 years who were eligible for health care services in Ontario, Canada. Participants were identified using administrative health databases from Ontario between January 1, 1992, and December 31, 2019. A total of 131 516 women were included in the primary (matched) analysis. Women were followed up until December 31, 2021.
Exposures: Salpingectomy (with and without hysterectomy) vs no pelvic procedure (control condition) among women in the general population.
Main outcomes and measures: Women with a unilateral or bilateral salpingectomy in Ontario between April 1, 1992, and December 31, 2019, were matched 1:3 to women with no pelvic procedure from the general population. Cox proportional hazards regression models were used to estimate the hazard ratios (HRs) and 95% CIs for ovarian, fallopian tube, and peritoneal cancer combined.
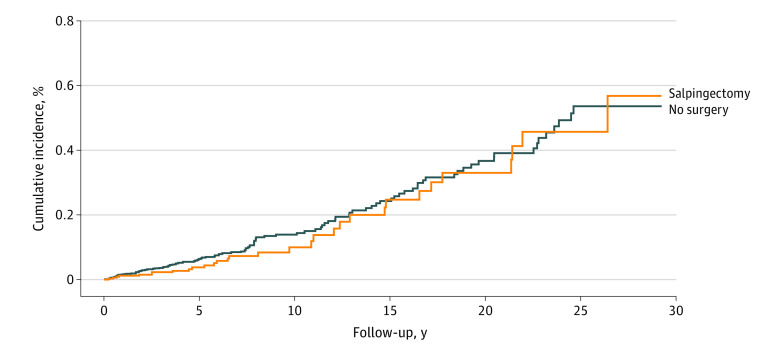
Results: Among 131 516 women (mean [SD] age, 42.2 [7.6] years), 32 879 underwent a unilateral or bilateral salpingectomy, and 98 637 did not undergo a pelvic procedure. After a mean (range) follow-up of 7.4 (0-29.2) years in the salpingectomy group and 7.5 (0-29.2) years in the nonsurgical control group, there were 31 incident cancers (0.09%) and 117 incident cancers (0.12%), respectively (HR, 0.82; 95% CI, 0.55-1.21). The HR for cancer incidence was 0.87 (95% CI, 0.53-1.44) when comparing those with salpingectomy vs those with hysterectomy alone.
Conclusions and relevance: In this cohort study, no association was found between salpingectomy and the risk of ovarian cancer; however, this observation was based on few incident cases and a relatively short follow-up time. Studies with additional years of follow-up are necessary to define the true level of potential risk reduction with salpingectomy, although longer follow-up will also be a challenge unless collaborative efforts that pool data are undertaken.
Conflict of interest statement
Figures
References
-
- Canadian Cancer Society; Canadian cancer statistics 2022. November 2022. Accessed March 2023. https://cancer.ca/en/research/cancer-statistics/canadian-cancer-statistics.
-
- Beral V, Doll R, Hermon C, Peto R, Reeves G; Collaborative Group on Epidemiological Studies of Ovarian Cancer . Ovarian cancer and oral contraceptives: collaborative reanalysis of data from 45 epidemiological studies including 23,257 women with ovarian cancer and 87,303 controls. Lancet. 2008;371(9609):303-314. doi:10.1016/S0140-6736(08)60167-1 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
