

Reconstructing the impact of COVID-19 on the immunity gap and transmission of respiratory syncytial virus in Lombardy, Italy
- PMID: 37566927
- PMCID: PMC10432612
- DOI: 10.1016/j.ebiom.2023.104745
Reconstructing the impact of COVID-19 on the immunity gap and transmission of respiratory syncytial virus in Lombardy, Italy
Abstract
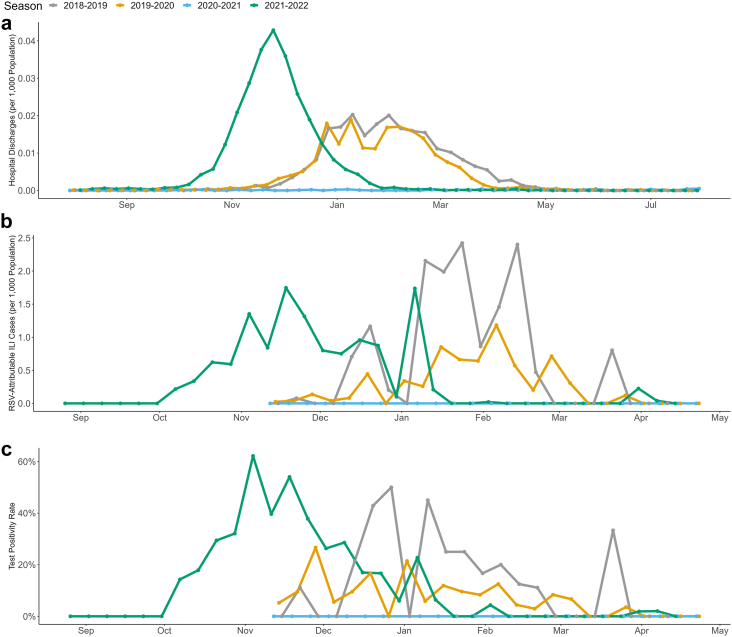
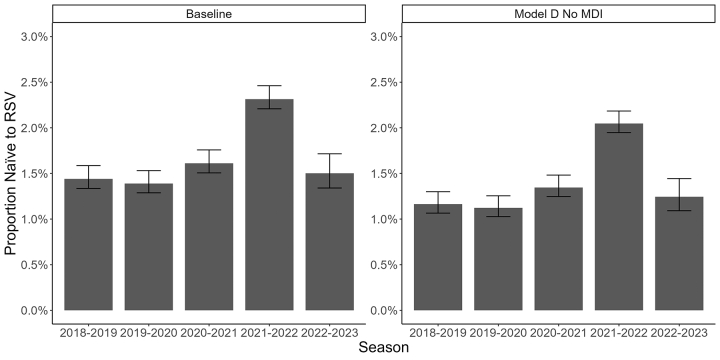
Background: Respiratory syncytial virus (RSV) is a leading cause of hospitalisation and mortality in young children globally. The social distancing measures implemented against COVID-19 in Lombardy (Italy) disrupted the typically seasonal RSV circulation during 2019-2021 and caused substantially more hospitalisations during 2021-2022. The primary aim of this study is to quantify the immunity gap-defined as the increased proportion of the population naïve to RSV infection following the relaxation of COVID-19 restrictions in Lombardy, which has been hypothesised to be a potential cause of the increased RSV burden in 2021-2022.
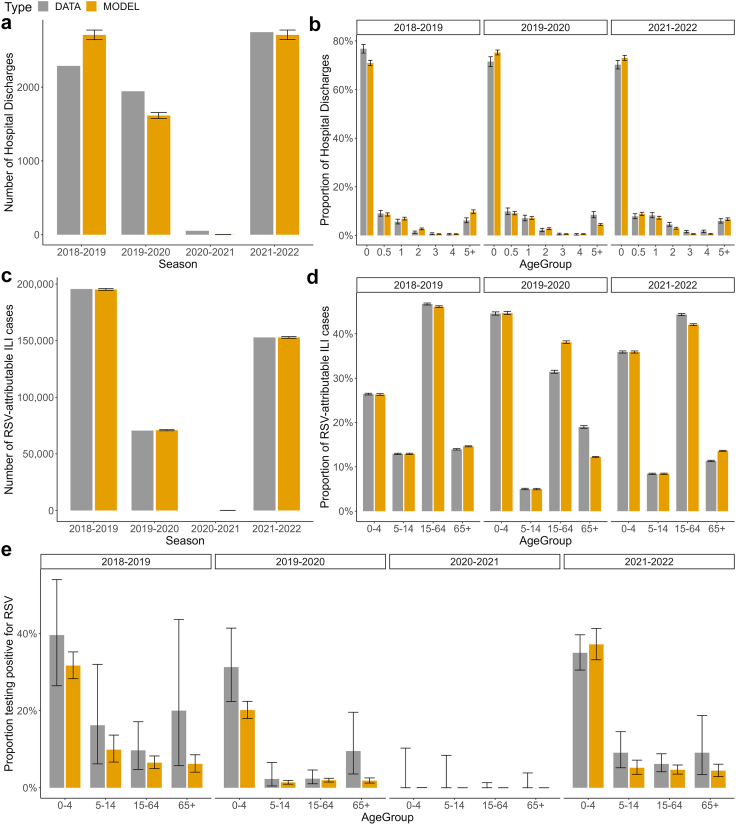
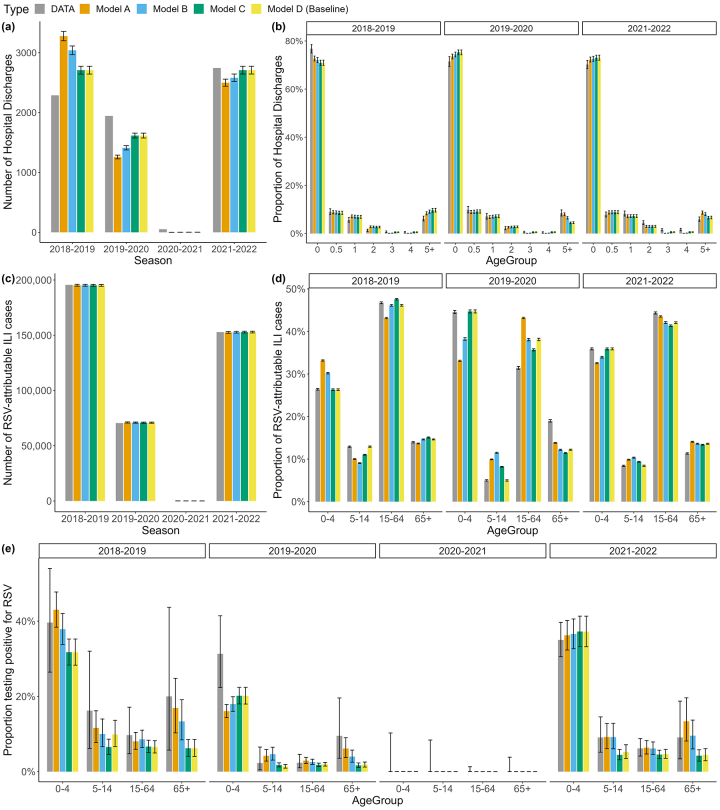
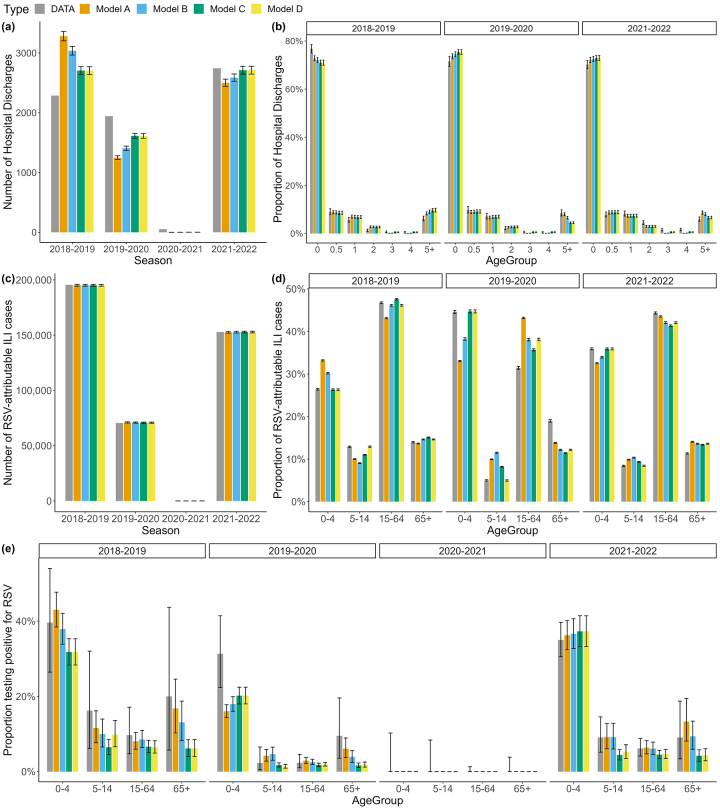
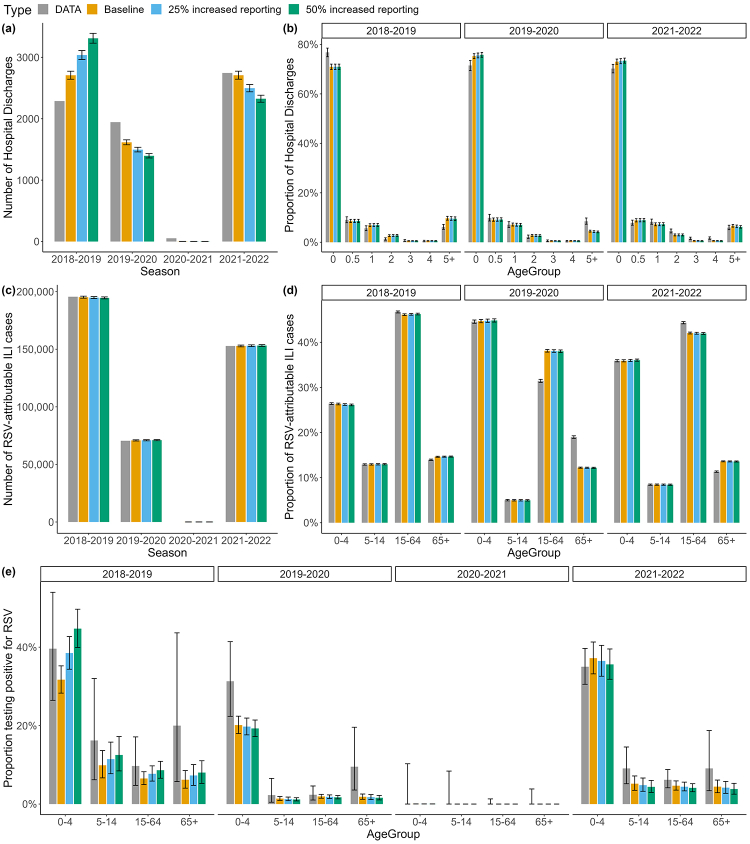
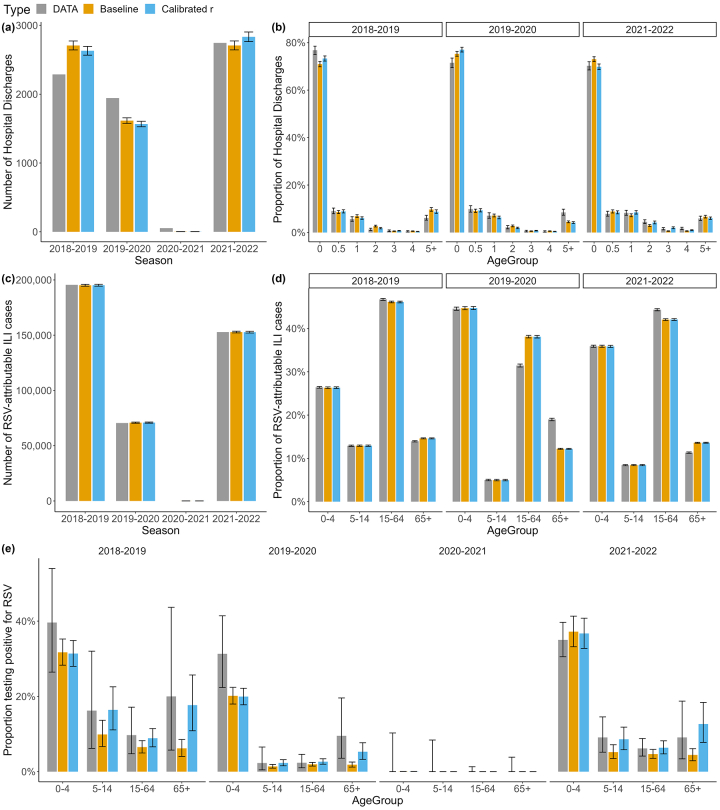
Methods: We developed a catalytic model to reconstruct changes in the age-dependent susceptibility profile of the Lombardy population throughout the COVID-19 pandemic. The model is calibrated to routinely collected hospitalisation, syndromic, and virological surveillance data and tested for alternative assumptions on age-dependencies in the risk of RSV infection throughout the pandemic.
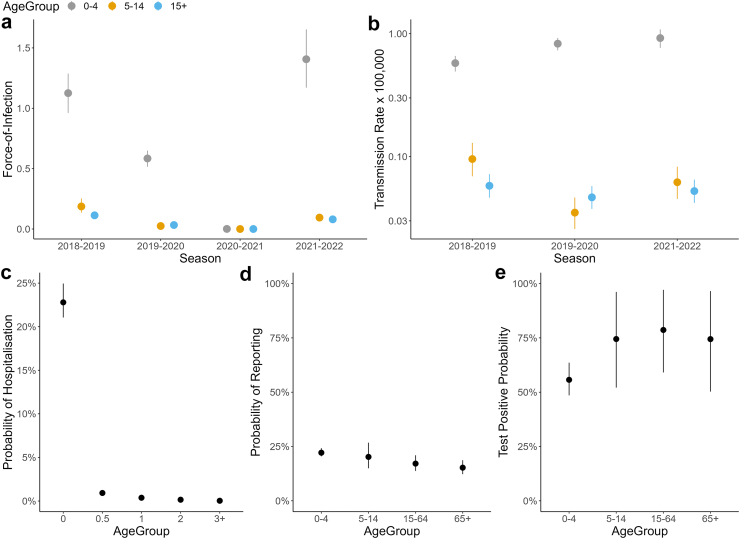
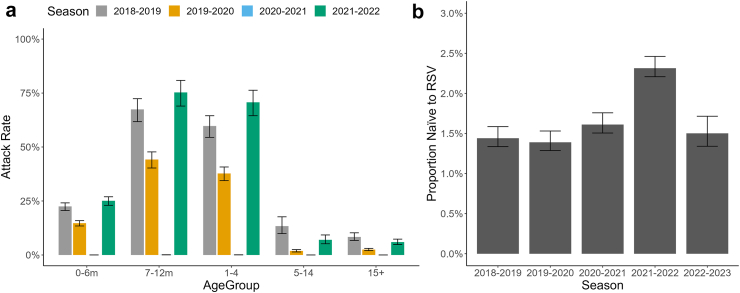
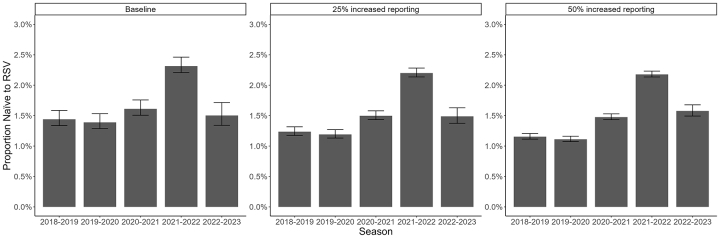
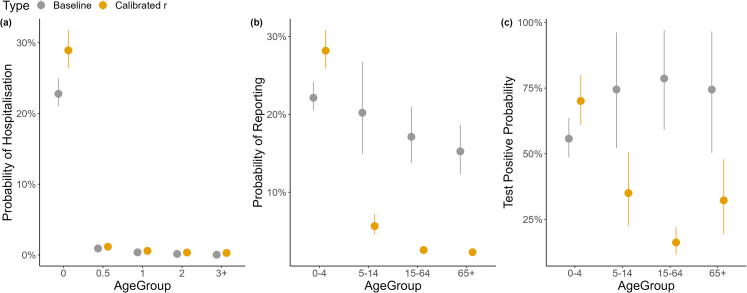
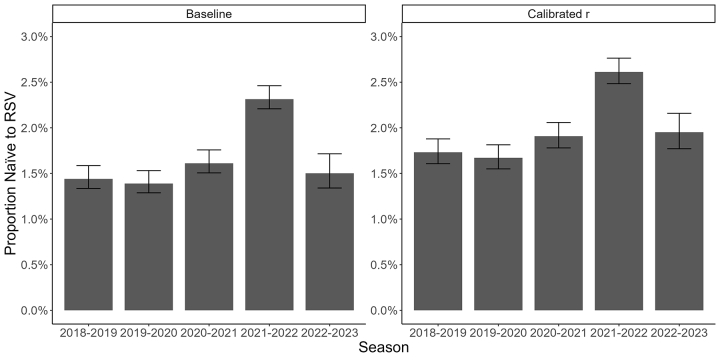
Findings: We estimate that the proportion of the Lombardy population naïve to RSV infection increased by 60.8% (95% CrI: 55.2-65.4%) during the COVID-19 pandemic: from 1.4% (95% CrI: 1.3-1.6%) in 2018-2019 to 2.3% (95% CrI: 2.2-2.5%) before the 2021-2022 season, corresponding to an immunity gap of 0.87% (95% CrI: 0.87-0.88%). We found evidence of heterogeneity in RSV transmission by age, suggesting that the COVID-19 restrictions had variable impact on the contact patterns and risk of RSV infection across ages.
Interpretation: We estimate a substantial increase in the population-level susceptibility to RSV in Lombardy during 2019-2021, which contributed to an increase in primary RSV infections in 2021-2022.
Funding: UK Medical Research Council (MRC), UK Foreign, Commonwealth & Development Office (FCDO), EDCTP2 programme, European Union, Wellcome Trust, Royal Society, EU-MUR PNRR INF-ACT.
Keywords: COVID-19 restrictions; Catalytic models; Immunity gap; Mathematical modelling; RSV.
Copyright © 2023 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures
References
-
- Li Y., Wang X., Blau D.M., et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. 2022 https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(22)00478... [cited 2022 May 23]. Available from: - PMC - PubMed
-
- Shi T., Denouel A., Tietjen A.K., et al. Global disease burden estimates of respiratory syncytial virus–associated acute respiratory infection in older adults in 2015: a systematic review and meta-analysis. J Infect Dis. 2020;222(Supplement_7):S577–S583. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
