

Variation in the stringency of COVID-19 public health measures on self-reported health, stress, and overall wellbeing in Canada
- PMID: 37567870
- PMCID: PMC10421886
- DOI: 10.1038/s41598-023-39004-w
Variation in the stringency of COVID-19 public health measures on self-reported health, stress, and overall wellbeing in Canada
Abstract
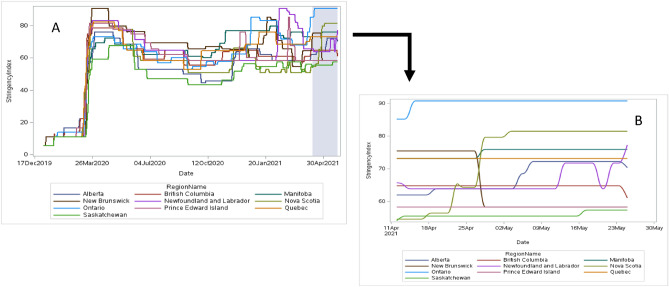
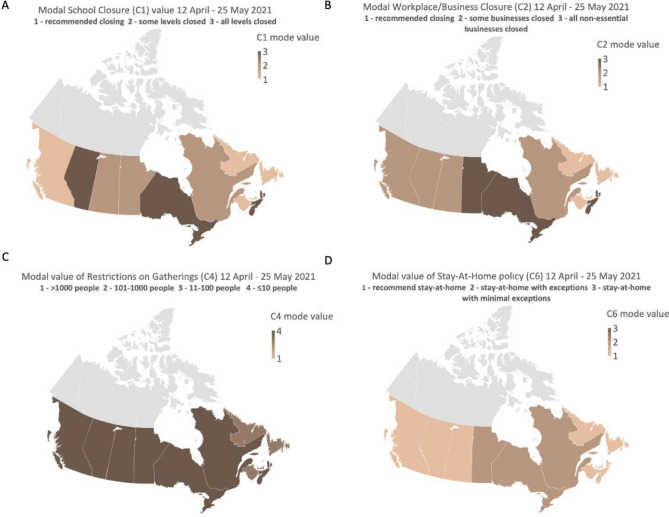
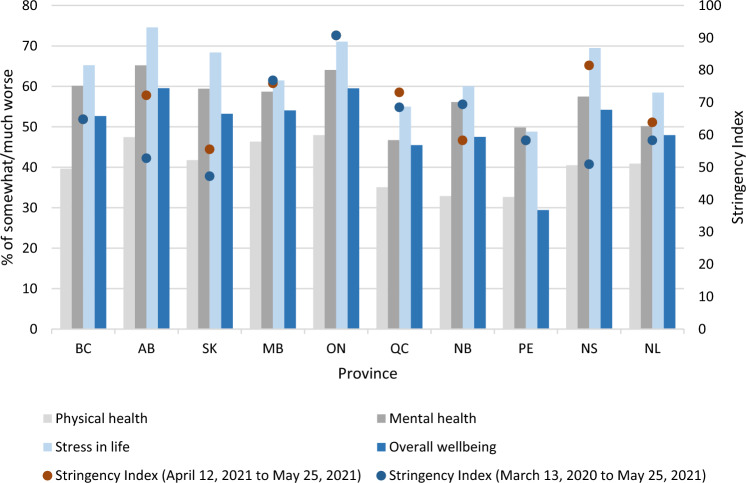
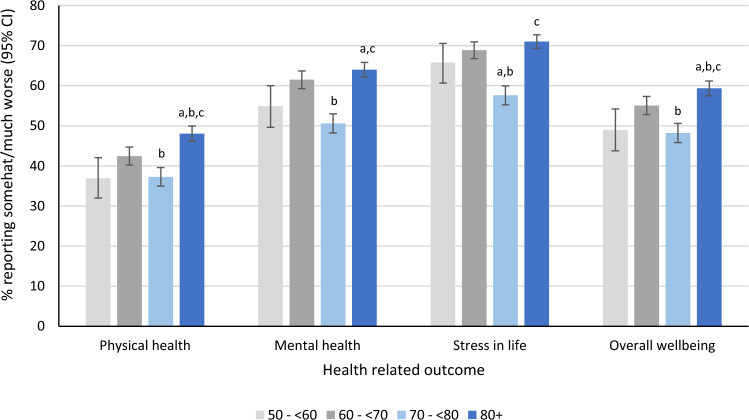
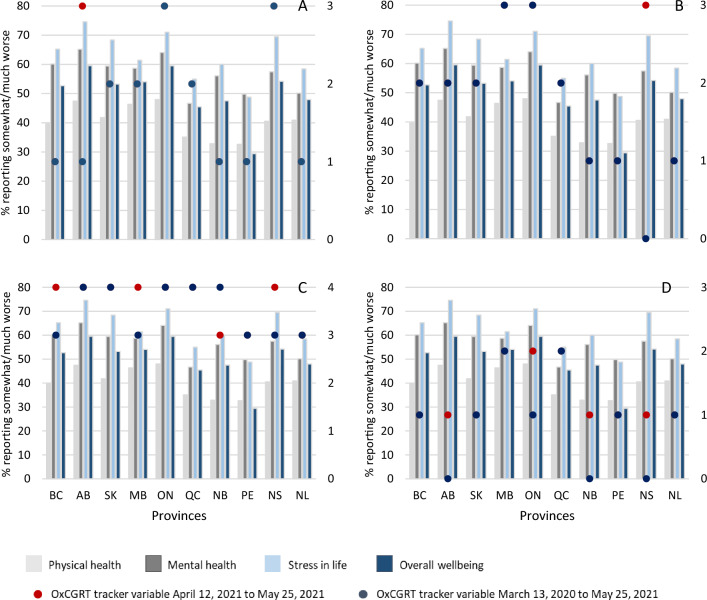
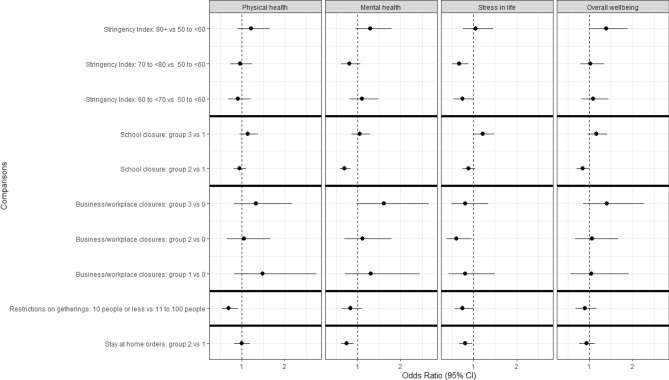
Evidence is building regarding the association between government implemented public health measures aimed at combating COVID-19 and their impacts on health. This study investigated the relationship between the stringency of public health measures implemented in Canada and self-reported mental health, physical health, stress, and wellbeing among a random sample of 6647 Canadians 18 years of age and older. The analysis was based on self-reported health data from the Canadian Perspectives on Environmental Noise Survey. This data was combined with the Oxford COVID-19 Government Response Tracker database, which included overall stringency index (SI), and four of its sub-components, i.e., school and business closures, restrictions on gatherings, and stay at home policies. Adjusted multivariate logistic regression models indicated that the magnitude of the overall SI was associated with higher or lower odds of reporting worse physical health, mental health, stress and/or overall wellbeing, depending on the measure evaluated. Similarly, policy directed at the four sub-components had varying impacts on the odds of reporting worse health, depending on the sub-component, the strength of the policy restriction, and the health outcome evaluated. The association between the strength of the public health measures and self-reported health, and how this may inform future policy, is discussed.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Statistics Canada (2020). Canadians report lower self-perceived mental health during the COVID-19 pandemic. Available at: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00003-eng... Accessed on 30 Nov 2021.
-
- Samji, H., et al. for the British Columbia Centre for Disease Control COVID-19 Young Adult Task Force. Impacts of the COVID-19 pandemic on the health and well-being of young adults in British Columbia. British Columbia Centre for Disease Control. Available at: http://www.bccdc.ca/Health-Professionals-Site/Documents/COVID-Impacts/BC... (2021).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
