

Clinical and Economic Benefit of Advanced Therapies for the Treatment of Active Ankylosing Spondylitis
- PMID: 37568031
- PMCID: PMC10468449
- DOI: 10.1007/s40744-023-00586-6
Clinical and Economic Benefit of Advanced Therapies for the Treatment of Active Ankylosing Spondylitis
Erratum in
-
Correction: Clinical and Economic Benefit of Advanced Therapies for the Treatment of Active Ankylosing Spondylitis.Rheumatol Ther. 2024 Feb;11(1):225-226. doi: 10.1007/s40744-023-00626-1. Rheumatol Ther. 2024. PMID: 38019452 Free PMC article. No abstract available.
Abstract
Introduction: Recent changes to treatment guidelines for ankylosing spondylitis (AS) have listed first-line advanced therapies as tumor necrosis factor (TNF), interleukin (IL)-17, and Janus kinase (JAK) inhibitors. This study sought to assess the comparative clinical and economic benefit of advanced therapies approved for AS.
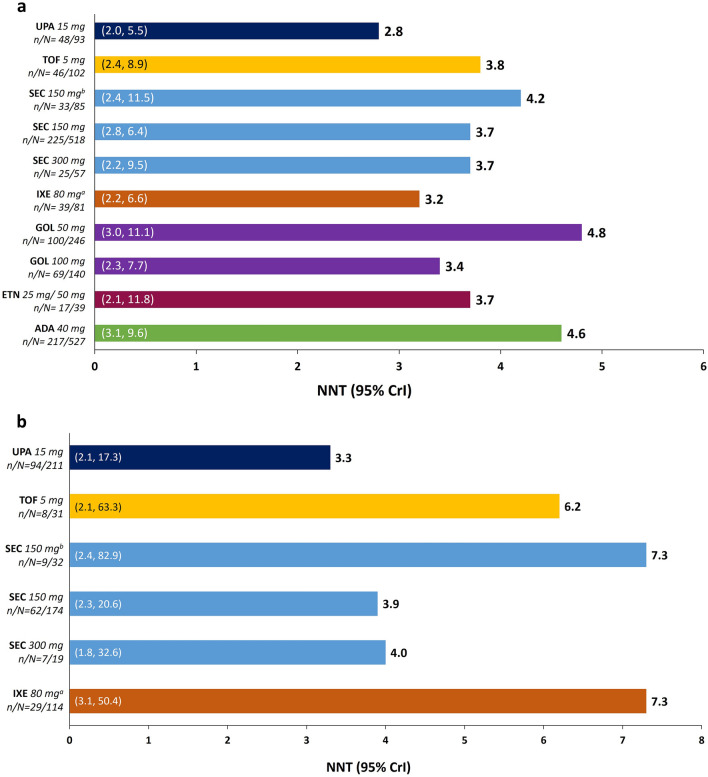
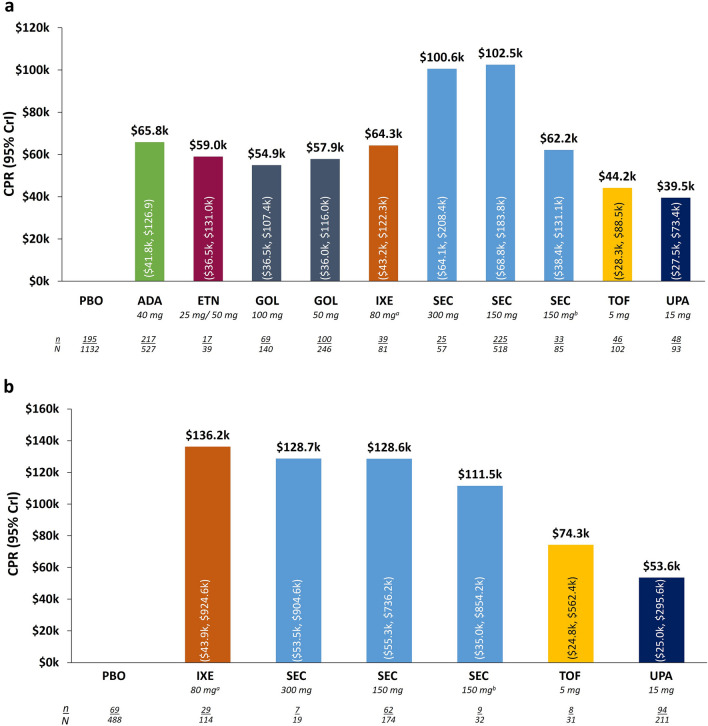
Methods: A systematic literature review was conducted to identify randomized clinical trials for JAK inhibitors (upadacitinib [UPA], tofacitinib [TOF]), anti-IL-17 therapies (secukinumab [SEC], ixekizumab [IXE]), and TNF inhibitors (adalimumab [ADA], etanercept [ETN], golimumab [GOL]) used for the treatment of active AS. Clinical efficacy was evaluated by Assessment of Spondyloarthritis International Society 40 (ASAS40) criteria and treatment discontinuation due to adverse events (AEs) was used to generate response rates synthesized via a Bayesian network meta-analysis. Number needed to treat (NNT) was calculated as the reciprocal of incremental response rate of each treatment versus placebo. Cost per ASAS40 responder (CPR) was calculated as the 12-week treatment costs divided by ASAS40 response rates. Data were stratified by biologic treatment status (i.e., biologic naïve [bio-naïve] or inadequate response or intolerance to biologics [bio-IR]) for efficacy and CPR analyses.
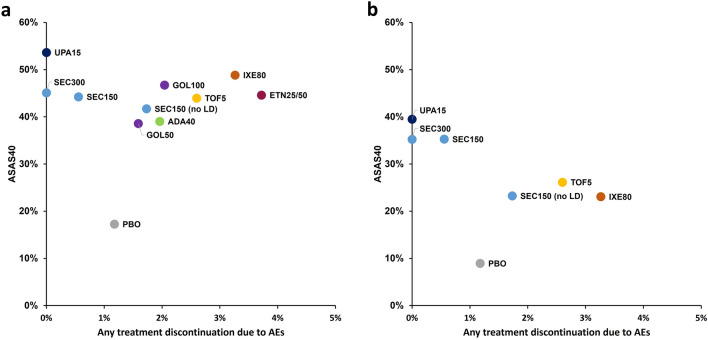
Results: Among bio-naïve patients, the response rate for ASAS40 was 53.6% for UPA-treated patients, whereas most other treatments had response rates between 41% and 49%. NNTs were lowest for UPA-treated patients at 2.8 (other therapies 3.2-4.8). Estimated CPR among UPA-treated patients was lowest (UPA $39.5k vs others $44.2k-102.5k). Efficacy and CPR trends were similar among bio-IR and TNF-IR patients. Among bio-naïve and bio-IR patients, the rate of AEs leading to discontinuation was lowest among UPA and SEC-treated patients (0.0, others 0.6-3.7%).
Conclusions: Relative to other treatments assessed in this study, UPA demonstrated numerically greater clinical and economic benefit for the treatment of AS. Head-to-head or real-world comparisons of these therapies are warranted and may inform clinical decision-making.
Keywords: Ankylosing spondylitis; Network meta-analysis; Treatment effectiveness; Upadacitinib.
© 2023. The Author(s).
Conflict of interest statement
Andrew Ostor has received consultant fees, acted on advisory boards, and participated in clinical trials for AbbVie, Janssen, Lilly, Novartis, Pfizer & GSK. Jessica A. Walsh has nothing to disclose. Christopher D Saffore is an employee of AbbVie Inc. and may hold stock. Eric B Collins is an employee of Medicus Economics LLC, which received consulting fees and research support from AbbVie.
Figures

References
-
- Ward MM, Deodhar A, Gensler LS, et al. Update of the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and treatment network recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Care Res (Hoboken) 2019;71(10):1285–1299. doi: 10.1002/acr.24025. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
