

Contextual sensory integration training vs. traditional vestibular rehabilitation: a pilot randomized controlled trial
- PMID: 37568216
- PMCID: PMC10422780
- DOI: 10.1186/s12984-023-01224-6
Contextual sensory integration training vs. traditional vestibular rehabilitation: a pilot randomized controlled trial
Abstract
Background: We created a clinical virtual reality application for vestibular rehabilitation. Our app targets contextual sensory integration (C.S.I.) where patients are immersed in safe, increasingly challenging environments while practicing various tasks (e.g., turning, walking). The purpose of this pilot study was to establish the feasibility of a randomized controlled trial comparing C.S.I. training to traditional vestibular rehabilitation.
Methods: Thirty patients with vestibular dysfunction completed the Dizziness Handicap Inventory (DHI), Activities-Specific Balance Confidence Scale (ABC), Visual Vertigo Analog Scale (VVAS), Functional Gait Assessment (FGA), Timed-Up-and-Go (TUG), and Four-Square Step Test (FSST). Following initial assessment, the patients were randomized into 8 weeks (once per week in clinic + home exercise program) of traditional vestibular rehabilitation or C.S.I. training. Six patients had to stop participation due to the covid-19 pandemic, 6 dropped out for other reasons (3 from each group). Ten patients in the traditional group and 8 in the C.S.I group completed the study. We applied an intention to treat analysis.
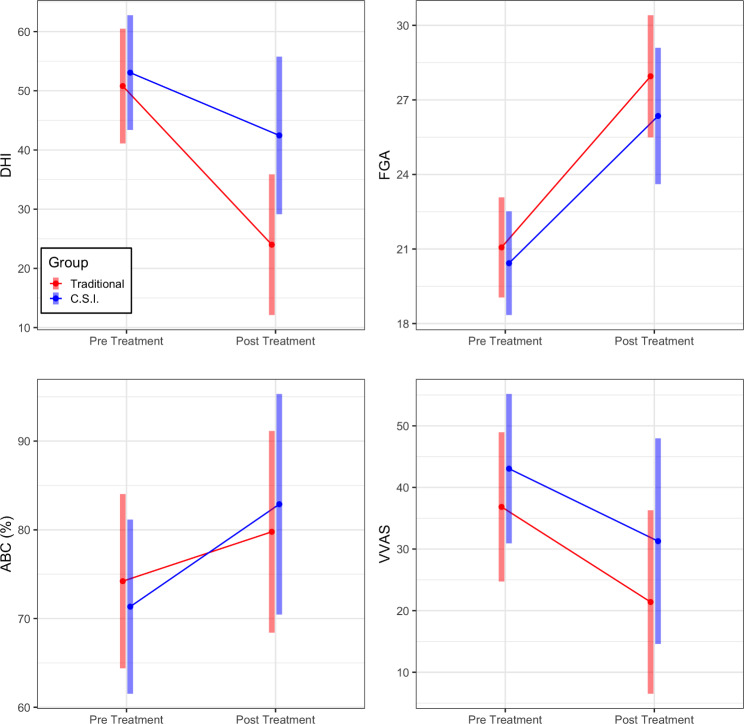
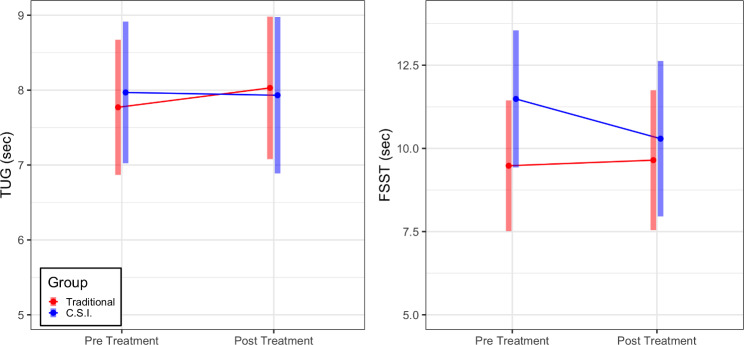
Results: Following intervention, we observed a significant main effect of time with no main effect of group or group by time interaction for the DHI (mean difference - 18.703, 95% CI [-28.235, -9.172], p = 0.0002), ABC (8.556, [0.938, 16.174], p = 0.028), VVAS, (-13.603, [-25.634, -1.573], p = 0.027) and the FGA (6.405, [4.474, 8.335], p < 0.0001). No changes were observed for TUG and FSST.
Conclusion: Patients' symptoms and function improved following either vestibular rehabilitation method. C.S.I training appeared comparable but not superior to traditional rehabilitation.
Trial registration: This study (NCT04268745) was registered on clincaltrials.gov and can be found at https://clinicaltrials.gov/ct2/show/NCT04268745 .
Keywords: Balance; HTC Vive; Head mounted Display; Vestibular Rehabilitation.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests. Prof. Perlin reported a research grant from Unity. Dr. Cosetti reported unpaid participation in research on cochlear implants and other implantable devices manufactured by Cochlear Americas, MED-El, and Oticon Medical. Neither is related to the submitted work.
Figures

References
-
- Hall CD, Herdman SJ, Whitney SL, Anson ER, Carender WJ, Hoppes CW, et al. Vestibular Rehabilitation for Peripheral vestibular hypofunction: an updated clinical practice Guideline from the Academy of neurologic physical therapy of the American Physical Therapy Association. J Neurol Phys Ther. 2022;46:118–77. doi: 10.1097/NPT.0000000000000382. - DOI - PMC - PubMed
-
- Sulway S, Whitney SL. Advances in vestibular Rehabilitation. Adv Otorhinolaryngol. 2019;82:164–9. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
