

Cardiologist-Directed Sedation Management in Patients Undergoing Transvenous Lead Extraction: A Single-Centre Retrospective Analysis
- PMID: 37568301
- PMCID: PMC10420171
- DOI: 10.3390/jcm12154900
Cardiologist-Directed Sedation Management in Patients Undergoing Transvenous Lead Extraction: A Single-Centre Retrospective Analysis
Abstract
Background: The demand for transvenous lead extraction (TLE) has increased. In line with this, the safety of such procedures has also increased. Traditionally, TLE is performed under resource-intensive general anaesthesia. This study aims to evaluate the safety and outcomes of Cardiologist-lead deep sedation for TLE.
Methods: We retrospectively analysed 328 TLE procedures performed under deep sedation from 2016 to 2019. TLE procedures were performed by experienced electrophysiologists. Sedation was administered by a specifically trained cardiologist (bolus midazolam/fentanyl and propofol infusion). Procedural sedation data including blood pressure, medication administration and sedation time were collected. Complications related to sedation and the operative component of the procedure were analysed retrospectively.
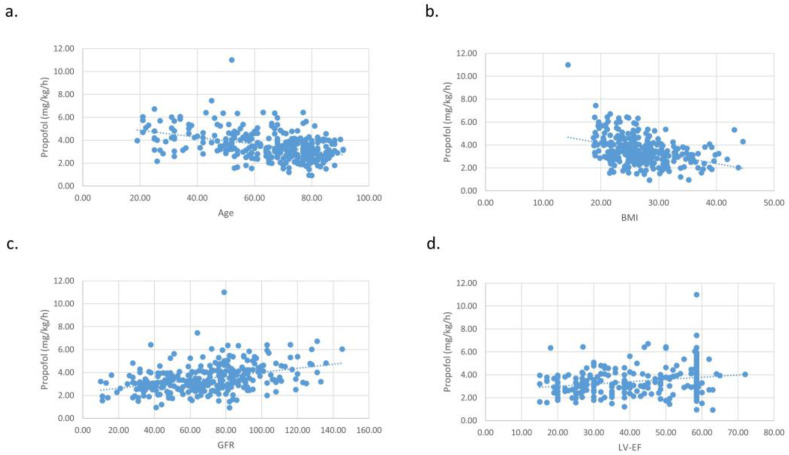
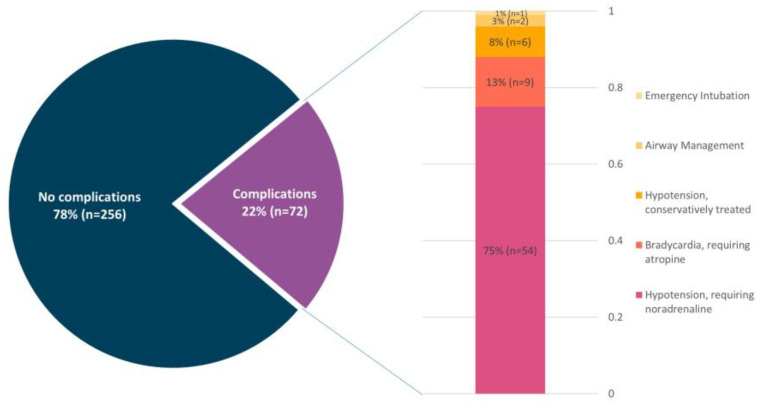
Results: The sedation-associated complication rate during TLE was 22.0%. The most common complication (75% of complications) was hypotension requiring noradrenaline, followed by bradycardia requiring atropine (13% of complications). Additionally, the unplanned presence of an anaesthesiologist was needed in one case (0.3%). Deep sedation was achieved with midazolam (mean dose 42.9 ± 26.5 µg/kg), fentanyl (mean dose 0.4 ± 0.6 µg/kg) and propofol (mean dose 3.5 ± 1.2 mg/kg/h). There was no difference in medication dosage between those with a sedation-associated complication and those without. Sedation-associated complications appeared significantly more in patients with reduced LVEF (p = 0.01), renal impairment (p = 0.01) and a higher American Society of Anaesthesiologists (ASA) class (p = 0.01).
Conclusion: Deep sedation for TLE can be safely performed by a specifically trained cardiologist, with a transition to general anaesthesia required in only 0.3% of cases. We continue to recommend the on-call availability of an anaesthesiologist and cardiac surgeon in case of major complications.
Keywords: cardiac implantable electronic devices; cardiologist-directed deep sedation; deep sedation; lead revision; transvenous lead extraction.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Kurtz S.M., Ochoa J.A., Lau E., Shkolnikov Y., Pavri B.B., Frisch D., Greenspon A.J. Implantation trends and patient profiles for pacemakers and implantable cardioverter defibrillators in the United States: 1993–2006. Pacing Clin. Electrophysiol. 2010;33:705–711. doi: 10.1111/j.1540-8159.2009.02670.x. - DOI - PubMed
-
- Greenspon A.J., Patel J.D., Lau E., Ochoa J.A., Frisch D.R., Ho R.T., Pavri B.B., Kurtz S.M. 16-Year trends in the infection burden for pacemakers and implantable cardioverter-defibrillators in the United States: 1993 to 2008. J. Am. Coll. Cardiol. 2011;58:1001–1006. doi: 10.1016/j.jacc.2011.04.033. - DOI - PubMed
-
- Schwarzwald S.N., Kersten D.J., Shaikh Z.A., Needelman B.S., Feldman A.M., Germano J., Islam S., Cohen T.J. Mechanisms of Lead Failure by Recall Status and Manufacturer: Results From the Pacemaker and Implantable Defibrillator Leads Survival Study (“PAIDLESS”) J. Invasive Cardiol. 2018;30:147–151. - PubMed
-
- Zabek A., Malecka B., Haberka K., Boczar K., Pfitzner R., Debski M., Lelakowski J. The analysis of indications and early results of transvenous lead extraction in patients with a pacemaker, ICD and CRT—Single-center experience. Acta Cardiol. 2015;70:685–692. doi: 10.1080/AC.70.6.3120181. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
