

Management of Acute Cholecystitis in High-Risk Patients: Percutaneous Gallbladder Drainage as a Definitive Treatment vs. Emergency Cholecystectomy-Systematic Review and Meta-Analysis
- PMID: 37568306
- PMCID: PMC10419867
- DOI: 10.3390/jcm12154903
Management of Acute Cholecystitis in High-Risk Patients: Percutaneous Gallbladder Drainage as a Definitive Treatment vs. Emergency Cholecystectomy-Systematic Review and Meta-Analysis
Abstract
Background: This systematic review aims to investigate whether percutaneous transhepatic gallbladder biliary drainage (PTGBD) is superior to emergency cholecystectomy (EC) as a definitive treatment in high-risk patients with acute cholecystitis (AC).
Material and methods: A systematic literature search was performed until December 2022 using the Scopus, Medline/PubMed and Web of Science databases.
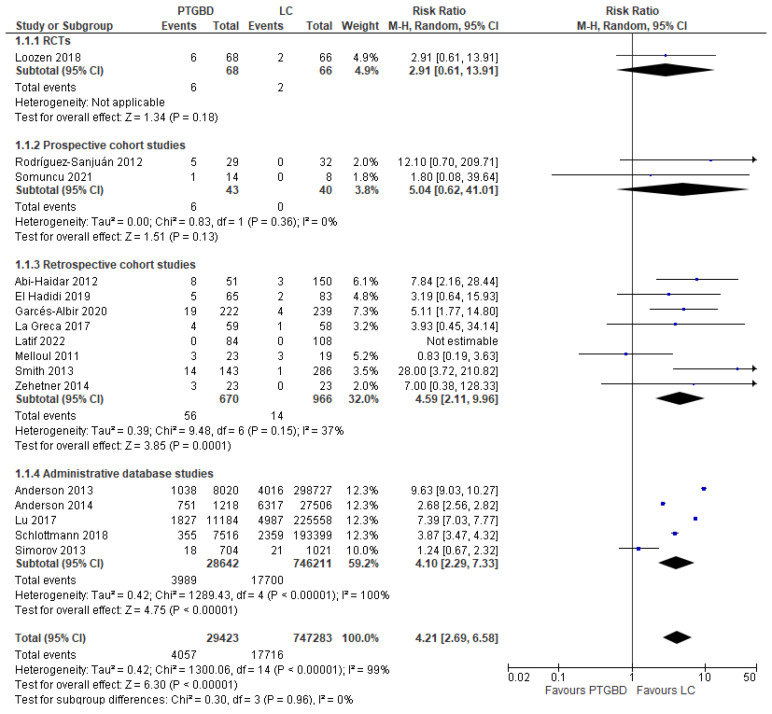
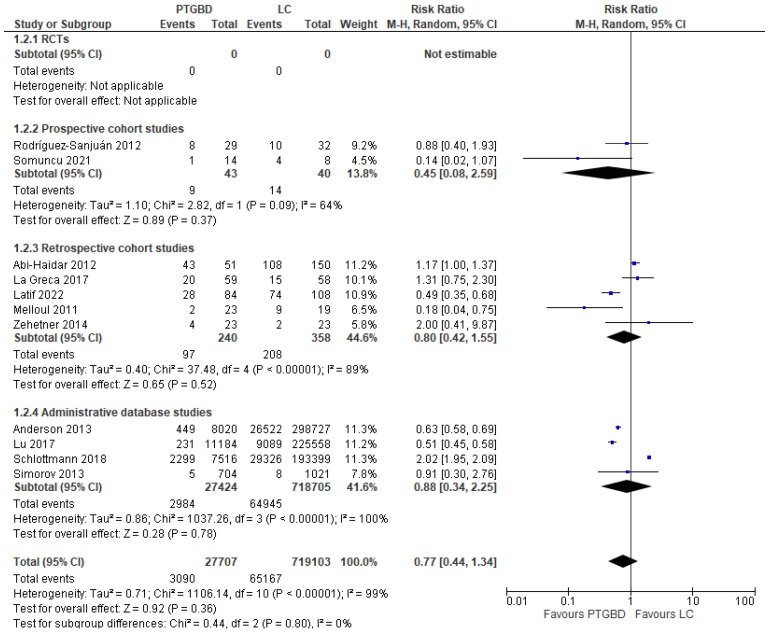
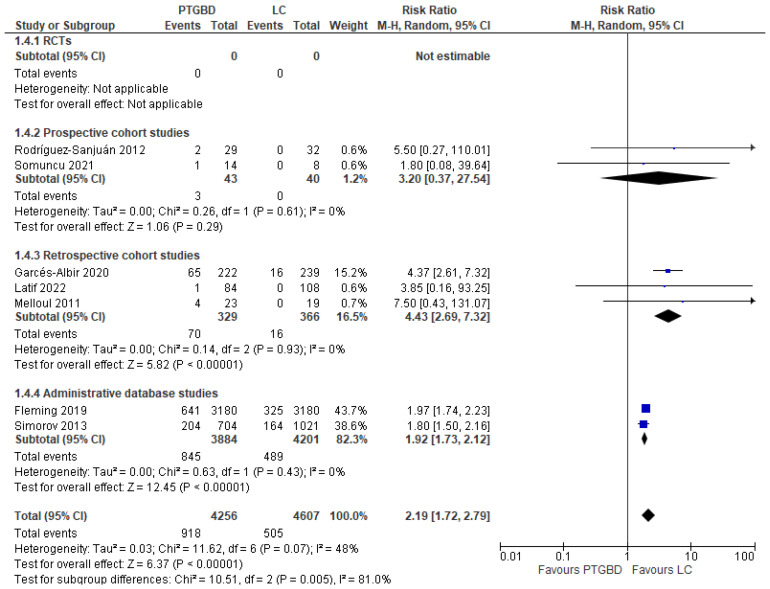
Results: Seventeen studies have been included with a total of 783,672 patients (32,634 treated with PTGBD vs. 4663 who underwent laparoscopic cholecystectomy, 343 who had open cholecystectomy and 746,032 who had some form of cholecystectomy, but without laparoscopic or open approach being specified). An analysis of the results shows that PTGBD, despite being less invasive, is not associated with lower morbidity with respect to EC (RR 0.77 95% CI [0.44 to 1.34]; I2 = 99%; p = 0.36). A lower postoperative mortality was reported in patients who underwent EC (2.37%) with respect to the PTGBD group (13.78%) (RR 4.21; 95% CI [2.69 to 6.58]; p < 0.00001); furthermore, the risk of hospital readmission for biliary complications (RR 2.19 95% CI [1.72 to 2.79]; I2 = 48%; p < 0.00001) and hospital stay (MD 4.29 95% CI [2.40 to 6.19]; p < 0.00001) were lower in the EC group.
Conclusions: In our systematic review, the majority of studies have very low-quality evidence and more RCTs are needed; furthermore, PTGBD is inferior in the treatment of AC in high-risk patients. The definition of high-risk patients is important in interpreting the results, but the methods of assessment and definitions differ between studies. The results of our systematic review and meta-analysis failed to demonstrate any advantage of using PTGBD over ER as a definitive treatment of AC in critically ill patients, which suggests that EC should be considered as the treatment of choice even in very high-risk patients. Most likely, the inferiority of PTGBD versus early LC for high-risk patients is related to an association of various patient-side factor conditions and the severity of acute cholecystitis.
Keywords: acute cholecystitis; cholecystectomy; cholecystostomy; cholecystostomy tube; gallbladder drain; gallbladder tube; laparoscopic cholecystectomy; open cholecystectomy; percutaneous cholecystectomy; severe cholecystitis; transhepatic gallbladder drain; transhepatic gallbladder tube.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
