

A Comprehensive Review on Neuroendocrine Neoplasms: Presentation, Pathophysiology and Management
- PMID: 37568540
- PMCID: PMC10420169
- DOI: 10.3390/jcm12155138
A Comprehensive Review on Neuroendocrine Neoplasms: Presentation, Pathophysiology and Management
Abstract
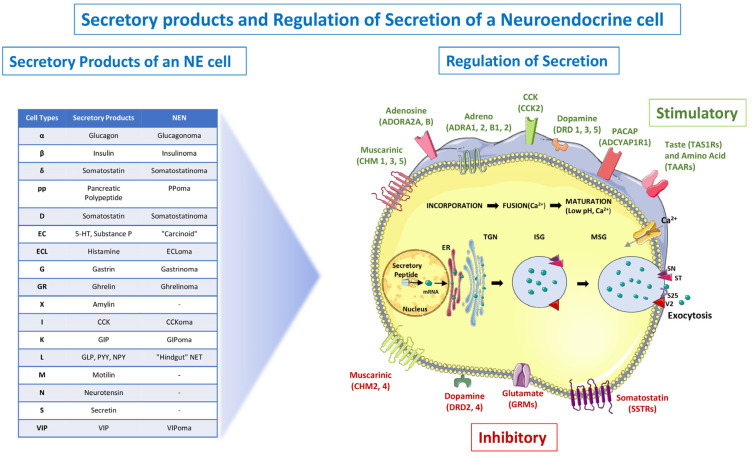
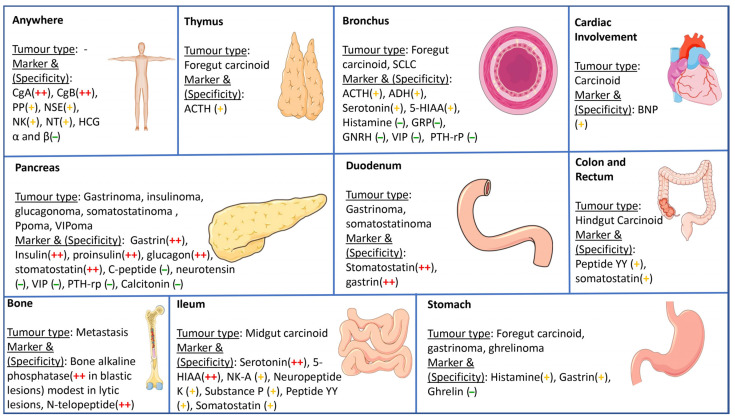
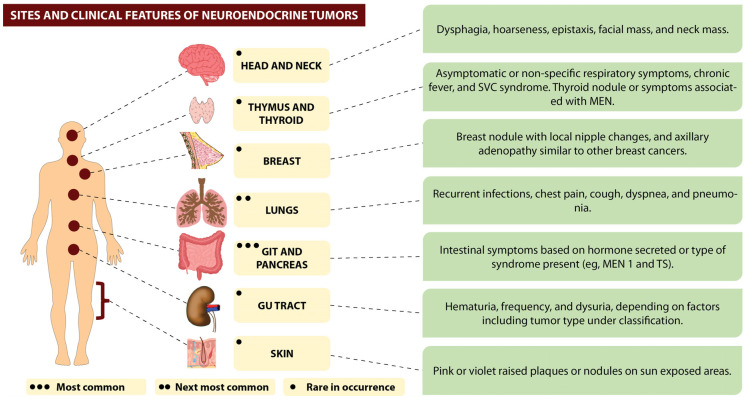
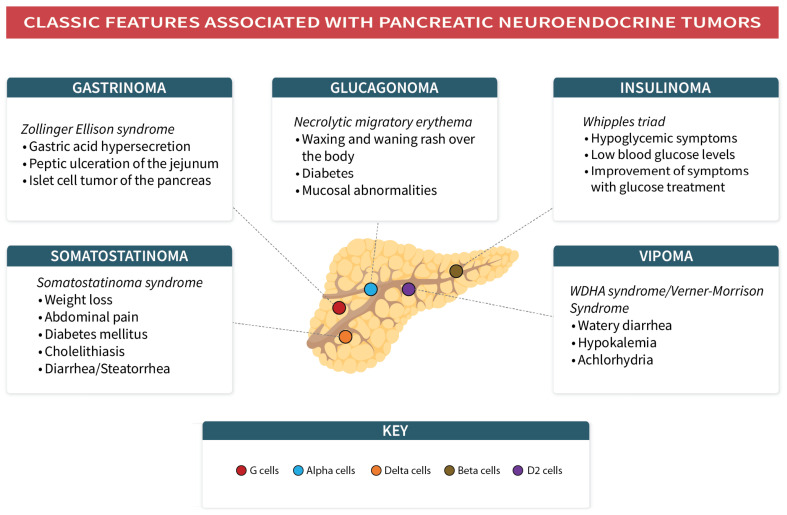
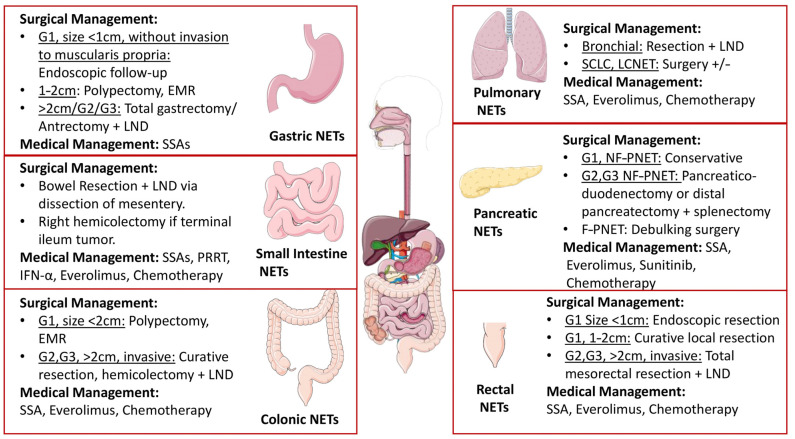
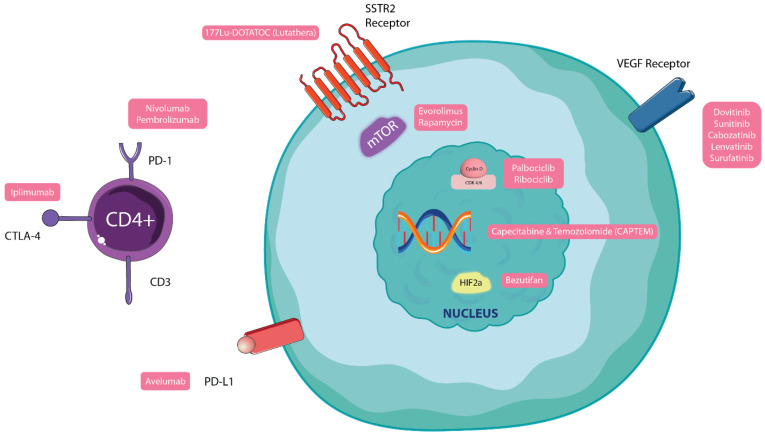
Neuroendocrine neoplasms (NENs) are a group of heterogeneous tumors with neuroendocrine differentiation that can arise from any organ. They account for 2% of all malignancies in the United States. A significant proportion of NEN patients experience endocrine imbalances consequent to increased amine or peptide hormone secretion, impacting their quality of life and prognosis. Over the last decade, pathologic categorization, diagnostic techniques and therapeutic choices for NENs-both well-differentiated neuroendocrine tumors (NETs) and poorly differentiated neuroendocrine carcinomas (NECs)-have appreciably evolved. Diagnosis of NEN mostly follows a suspicion from clinical features or incidental imaging findings. Hormonal or non-hormonal biomarkers (like serum serotonin, urine 5-HIAA, gastrin and VIP) and histology of a suspected NEN is, therefore, critical for both confirmation of the diagnosis and classification as an NET or NEC. Therapy for NENs has progressed recently based on a better molecular understanding, including the involvement of mTOR, VEGF and peptide receptor radionuclide therapy (PRRT), which add to the growing evidence supporting the possibility of treatment beyond complete resection. As the incidence of NENs is on the rise in the United States and several other countries, physicians are more likely to see these cases, and their better understanding may support earlier diagnosis and tailoring treatment to the patient. We have compiled clinically significant evidence for NENs, including relevant changes to clinical practice that have greatly updated our diagnostic and therapeutic approach for NEN patients.
Keywords: carcinoid syndrome; gastroenteropancreatic neuroendocrine tumors; neuroendocrine carcinomas; neuroendocrine tumors; pulmonary neuroendocrine tumors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Yao J.C., Hassan M.M., Phan A.T., Dagohoy C.G., Leary C., Mares J.E., Abdalla E.K., Fleming J.B., Vauthey J.N., Rashid A., et al. One Hundred Years after “Carcinoid”: Epidemiology of and Prognostic Factors for Neuroendocrine Tumors in 35,825 Cases in the United States. J. Clin. Oncol. 2008;26:3063–3072. doi: 10.1200/JCO.2007.15.4377. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
