

Radical Tumor Denervation Activates Potent Local and Global Cancer Treatment
- PMID: 37568574
- PMCID: PMC10417359
- DOI: 10.3390/cancers15153758
Radical Tumor Denervation Activates Potent Local and Global Cancer Treatment
Abstract
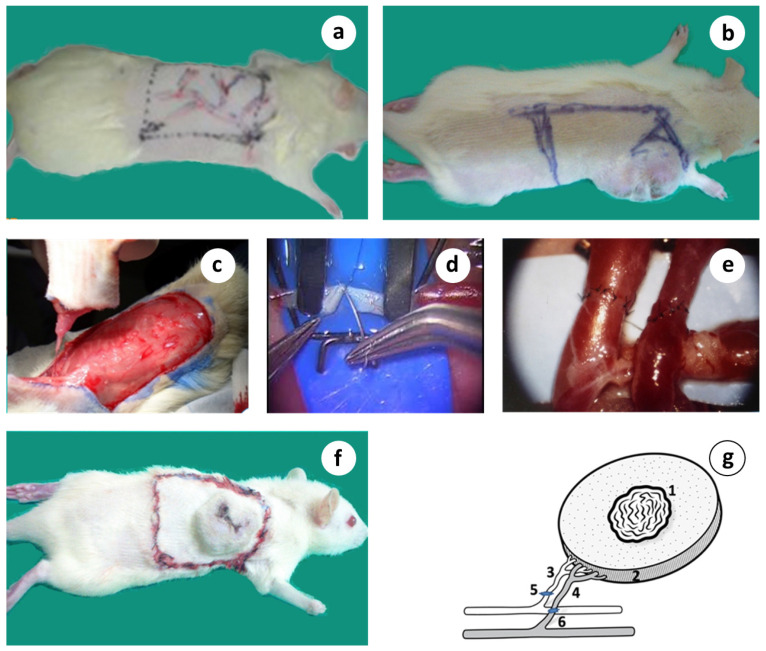
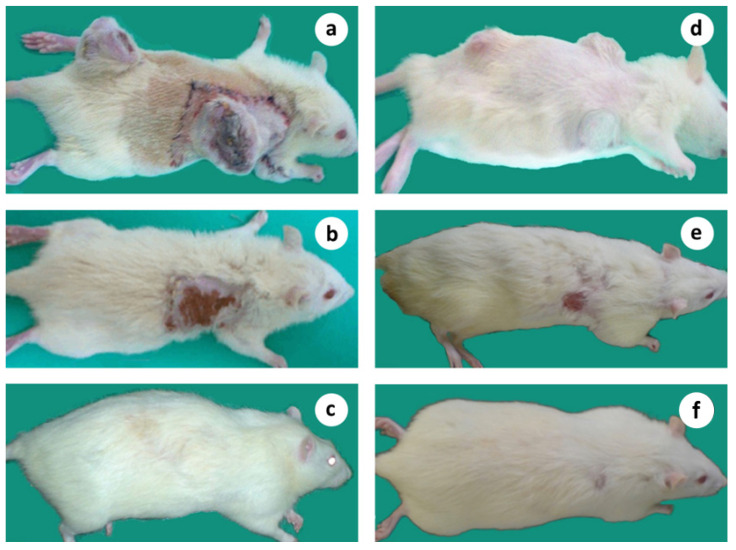
This preliminary study seeks to determine the effect of R&P denervation on tumor growth and survival in immunocompetent rats bearing an aggressive and metastatic breast solid tumor. A novel microsurgical approach was applied "in situ", aiming to induce R&P denervation through the division of every single nerve fiber connecting the host with the primary tumor via its complete detachment and re-attachment, by resecting and reconnecting its supplying artery and vein (anastomosis). This preparation, known as microsurgical graft or flap, is radically denervated by definition, but also effectively delays or even impedes the return of innervation for a significant period of time, thus creating a critical and therapeutic time window. Mammary adenocarcinoma cells (HH-16.cl4) were injected into immunocompetent Sprague Dawley adult rats. When the tumors reached a certain volume, the subjects entered the study. The primary tumor, including a substantial amount of peritumoral tissue, was surgically isolated on a dominant artery and vein, which was resected and reconnected using a surgical microscope (orthotopic tumor auto-transplantation). Intending to simulate metastasis, two or three tumors were simultaneously implanted and only one was treated, using the surgical technique described herein. Primary tumor regression was observed in all of the microsurgically treated subjects, associated with a potent systemic anticancer effect and prolonged survival. In stark contrast, the subjects received a close to identical surgical operation; however, with the intact neurovascular connection, they did not achieve the therapeutic result. Animals bearing multiple tumors and receiving the same treatment in only one tumor exhibited regression in both the "primary" and remote- untreated tumors at a clinically significant percentage, with regression occurring in more than half of the treated subjects. A novel therapeutic approach is presented, which induces the permanent regression of primary and, notably, remote tumors, as well as, evidently, the naturally occurring metastatic lesions, at a high rate. This strategy is aligned with the impetus that comes from the current translational research data, focusing on the abrogation of the neuro-tumoral interaction as an alternative treatment strategy. More data regarding the clinical significance of this are expected to come up from a pilot clinical trial that is ongoing.
Keywords: abscopal effect; cancer neurobiology; microsurgery; radical denervation; tumor denervation; tumor regression.
Conflict of interest statement
There are no financial conflict of interest to disclose.
Figures










References
-
- Patterson J.T., Olson J.S. The History of Cancer: An Annotated Bibliography. J. Am. Hist. 1991;77:1475. doi: 10.2307/2078448. - DOI
LinkOut - more resources
Full Text Sources
