

Preoperative Radiotherapy with a Simultaneous Integrated Boost Compared to Chemoradiotherapy for cT3-4 Rectal Cancer: Long-Term Results of a Multicenter Randomized Study
- PMID: 37568685
- PMCID: PMC10416952
- DOI: 10.3390/cancers15153869
Preoperative Radiotherapy with a Simultaneous Integrated Boost Compared to Chemoradiotherapy for cT3-4 Rectal Cancer: Long-Term Results of a Multicenter Randomized Study
Abstract
Background: Preoperative chemoradiotherapy (CRT) is the standard treatment for T3-4 rectal cancer. Here, we compared image-guided and intensity-modulated RT (IG-IMRT) with a simultaneous integrated boost (SIB) (instead of concomitant chemotherapy) versus CRT in a multi-centric randomized trial.
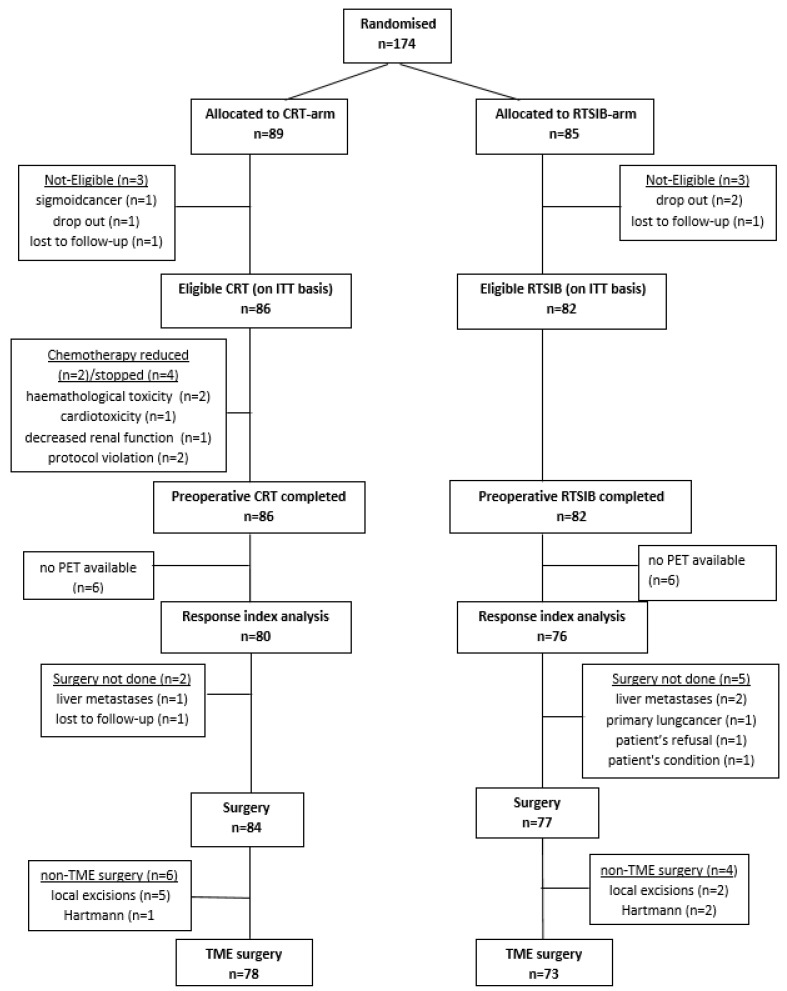
Methods: cT3-4 rectal cancer patients were randomly assigned to receive preoperative IG-IMRT 46 Gy/23 fractions plus capecitabine 825 mg/m² twice daily (CRT arm) or IG-IMRT 46 Gy/23 fractions with an SIB to the rectal tumor up to a total dose of 55.2 Gy (RTSIB arm).
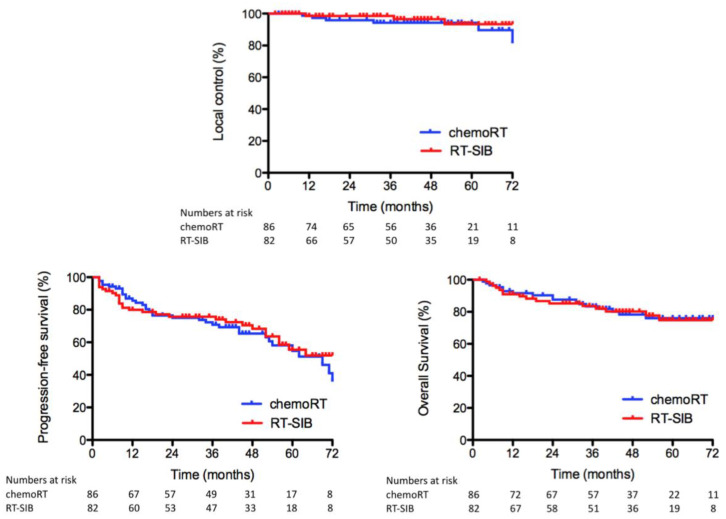
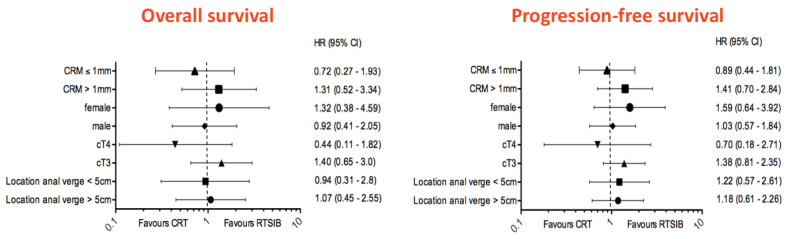
Results: A total of 174 patients were randomly assigned between April 2010 and May 2014. Grade 3 acute toxicities were 6% and 4% in the CRT and RTSIB arms, respectively. The mean fractional change in SUVmax at 5 weeks after completion of preoperative RT were -55.8% (±24.0%) and -52.9% (±21.6%) for patients in the CRT arm and RTSIB arm, respectively (p = 0.43). The pathologic complete response rate was 24% with CRT compared to 14% with RTSIB. There were no differences in 5-year overall survival (OS), progression-free survival (PFS) or local control (LC).
Conclusions: The preoperative RTSIB approach was not inferior to CRT in terms of metabolic response, toxicity, OS, PFS and LC, and could be considered an available option for patients unfit for fluorouracil-based CRT.
Keywords: chemoradiotherapy (CRT); image-guided and intensity-modulated RT (IG-IMRT); radiation therapy; randomized clinical trial; rectal cancer; simultaneous integrated boost (SIB).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Gérard J.P., Conroy T., Bonnetain F., Bouché O., Chapet O., Closon-Dejardin M.T., Untereiner M., Leduc B., Francois E., Maurel J., et al. Preoperative radiotherapy with or without concurrent fluorouracil and leucovorin in T3-4 rectal cancers: Results of FFCD 9203. J. Clin. Oncol. 2006;24:4620–4625. doi: 10.1200/JCO.2006.06.7629. - DOI - PubMed
-
- De Ridder M., Tournel K., Van Nieuwenhove Y., Engels B., Hoorens A., Everaert H., Op de Beeck B., Vinh-Hung V., De Grève J., Delvaux G., et al. Phase II study of preoperative helical tomotherapy for rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008;70:728–734. doi: 10.1016/j.ijrobp.2007.07.2332. - DOI - PubMed
-
- Engels B., Tournel K., Everaert H., Hoorens A., Sermeus A., Christian N., Storme G., Verellen D., De Ridder M. Phase II study of preoperative helical tomotherapy with a simultaneous integrated boost for rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012;83:142–148. doi: 10.1016/j.ijrobp.2011.05.068. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
