

Promise and Challenges of T Cell Immunotherapy for Osteosarcoma
- PMID: 37569894
- PMCID: PMC10419531
- DOI: 10.3390/ijms241512520
Promise and Challenges of T Cell Immunotherapy for Osteosarcoma
Abstract
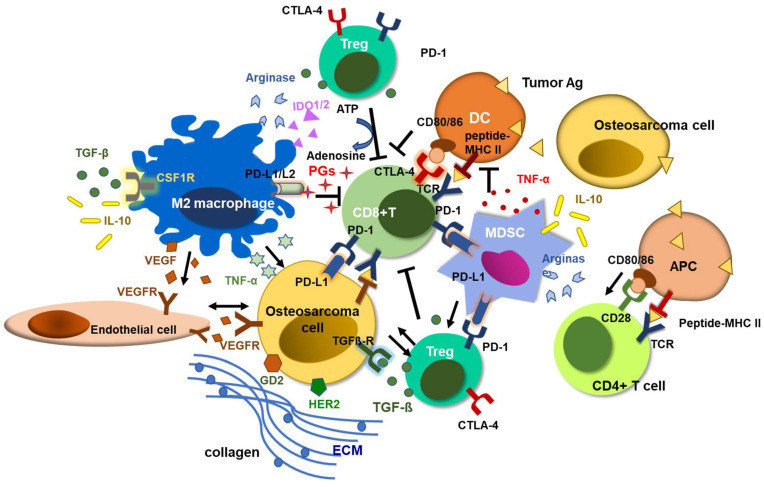
The cure rate for metastatic or relapsed osteosarcoma has not substantially improved over the past decades despite the exploitation of multimodal treatment approaches, allowing long-term survival in less than 30% of cases. Patients with osteosarcoma often develop resistance to chemotherapeutic agents, where personalized targeted therapies should offer new hope. T cell immunotherapy as a complementary or alternative treatment modality is advancing rapidly in general, but its potential against osteosarcoma remains largely unexplored. Strategies incorporating immune checkpoint inhibitors (ICIs), chimeric antigen receptor (CAR) modified T cells, and T cell engaging bispecific antibodies (BsAbs) are being explored to tackle relapsed or refractory osteosarcoma. However, osteosarcoma is an inherently heterogeneous tumor, both at the intra- and inter-tumor level, with no identical driver mutations. It has a pro-tumoral microenvironment, where bone cells, stromal cells, neovasculature, suppressive immune cells, and a mineralized extracellular matrix (ECM) combine to derail T cell infiltration and its anti-tumor function. To realize the potential of T cell immunotherapy in osteosarcoma, an integrated approach targeting this complex ecosystem needs smart planning and execution. Herein, we review the current status of T cell immunotherapies for osteosarcoma, summarize the challenges encountered, and explore combination strategies to overcome these hurdles, with the ultimate goal of curing osteosarcoma with less acute and long-term side effects.
Keywords: T cell engaging bispecific antibody; T cell immunotherapy; chimeric antigen receptor; immune checkpoint inhibitors; myeloid-derived suppressor cells; osteosarcoma; tumor microenvironment; tumor-associated macrophage; vascular endothelial growth factor.
Conflict of interest statement
N.K.C. and J.A.P. both declare that this study received funding from the following institutions. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication. Both N.K.C. and J.A.P. were named as inventors on the patent of EATs filed by M.S.K. Both M.S.K. and N.K.C. have financial interest in Y-mAbs, Abpro-Labs and Eureka Therapeutics. N.K.C. reports receiving past commercial research grants from Y-mabs Therapeutics and Abpro-Labs Inc. N.K.C. was named as inventor on multiple patents filed by M.S.K., including those licensed to Ymabs Therapeutics, Biotec Pharmacon, and Abpro-labs. N.K.C. is a SAB member for Eureka Therapeutics.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
