

Trends in mortality after a sepsis hospitalization: a nationwide prospective registry study from 2008 to 2021
- PMID: 37572240
- PMCID: PMC10665235
- DOI: 10.1007/s15010-023-02082-z
Trends in mortality after a sepsis hospitalization: a nationwide prospective registry study from 2008 to 2021
Erratum in
-
Correction: Trends in mortality after a sepsis hospitalization: a nationwide prospective registry study from 2008 to 2021.Infection. 2023 Dec;51(6):1871-1873. doi: 10.1007/s15010-023-02090-z. Infection. 2023. PMID: 37735342 Free PMC article. No abstract available.
Abstract
Background: Few studies have reported on mortality beyond one year after sepsis. We aim to describe trends in short- and long-term mortality among patients admitted with sepsis, and to describe the association between clinical characteristics and mortality for improved monitoring, treatment and prognosis.
Methods: Patients ≥ 18 years admitted to all Norwegian hospitals (2008-2021) with a first sepsis episode were identified using Norwegian Patient Registry and International Classification of Diseases 10th Revision codes. Sepsis was classified as implicit (known infection site plus organ dysfunction), explicit (unknown infection site), or COVID-19-related sepsis. The outcome was all-cause mortality. We describe age-standardized 30-day, 90-day, 1-, 5- and 10-year mortality for each admission year and estimated the annual percentage change with 95% confidence interval (CI). The association between clinical characteristics and all-cause mortality is reported as hazard ratios (HRs) adjusted for age, sex and calendar year in Cox regression.
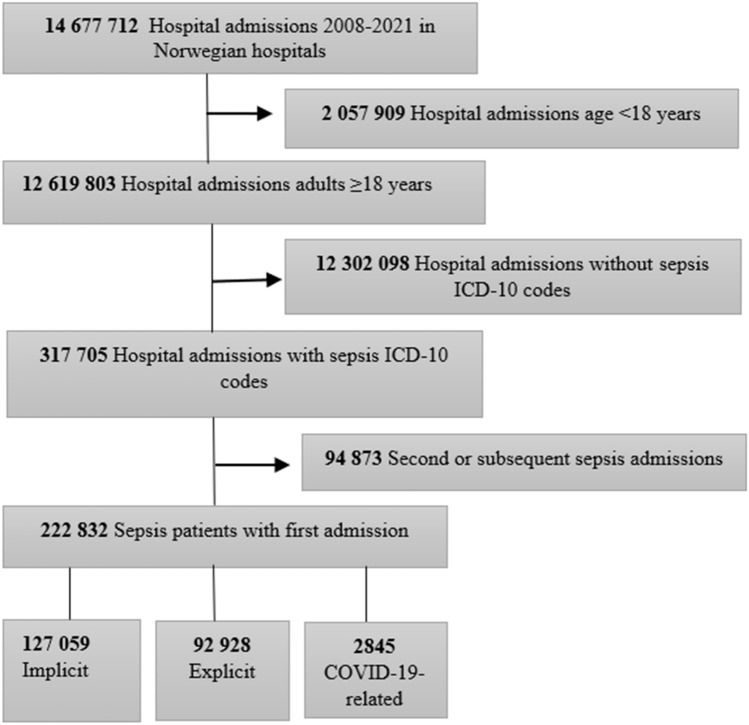
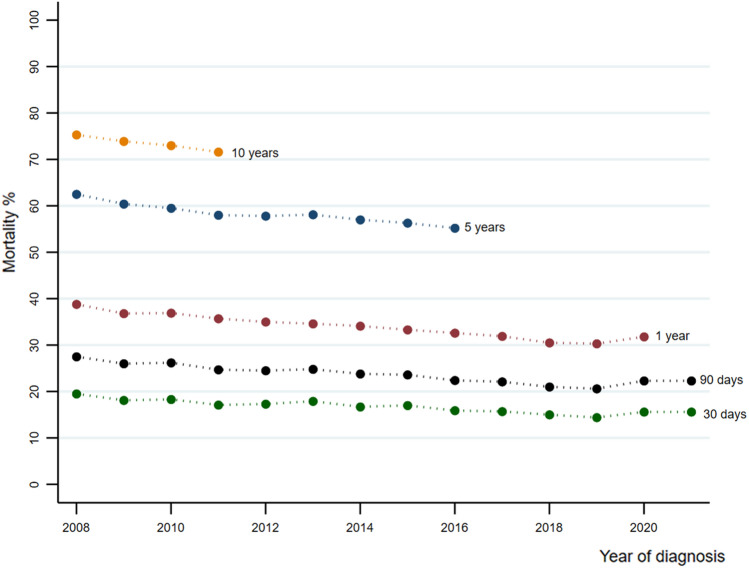
Results: The study included 222,832 patients, of whom 127,059 (57.1%) had implicit, 92,928 (41.7%) had explicit, and 2,845 (1.3%) had COVID-19-related sepsis (data from 2020 and 2021). Trends in overall age-standardized 30-day, 90-day, 1- and 5-year mortality decreased by 0.29 (95% CI - 0.39 to - 0.19), 0.43 (95% CI - 0.56 to - 0.29), 0.61 (95% CI - 0.73 to - 0.49) and 0.66 (95% CI - 0.84 to - 0.48) percent per year, respectively. The decrease was observed for all infections sites but was largest among patients with respiratory tract infections. Implicit, explicit and COVID-19-related sepsis had largely similar overall mortality, with explicit sepsis having an adjusted HR of 0.980 (95% CI 0.969 to 0.991) and COVID-19-related sepsis an adjusted HR of 0.916 (95% CI 0.836 to 1.003) compared to implicit sepsis. Patients with respiratory tract infections have somewhat higher mortality than those with other infection sites. Number of comorbidities was positively associated with mortality, but mortality varied considerably between different comorbidities. Similarly, number of acute organ dysfunctions was strongly associated with mortality, whereas the risk varied for each type of organ dysfunction.
Conclusion: Overall mortality has declined over the past 14 years among patients with a first sepsis admission. Comorbidity, site of infection, and acute organ dysfunction are patient characteristics that are associated with mortality. This could inform health care workers and raise the awareness toward subgroups of patients that needs particular attention to improve long-term mortality.
Keywords: COVID-19; Intensive care; Mortality; Sepsis.
© 2023. The Author(s).
Conflict of interest statement
None of the authors have any conflicts of interest to declare.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
