

Influence of arterial blood gases on the renal arterial resistive index in intensive care unit
- PMID: 37573336
- PMCID: PMC10423423
- DOI: 10.1186/s12967-023-04407-w
Influence of arterial blood gases on the renal arterial resistive index in intensive care unit
Abstract
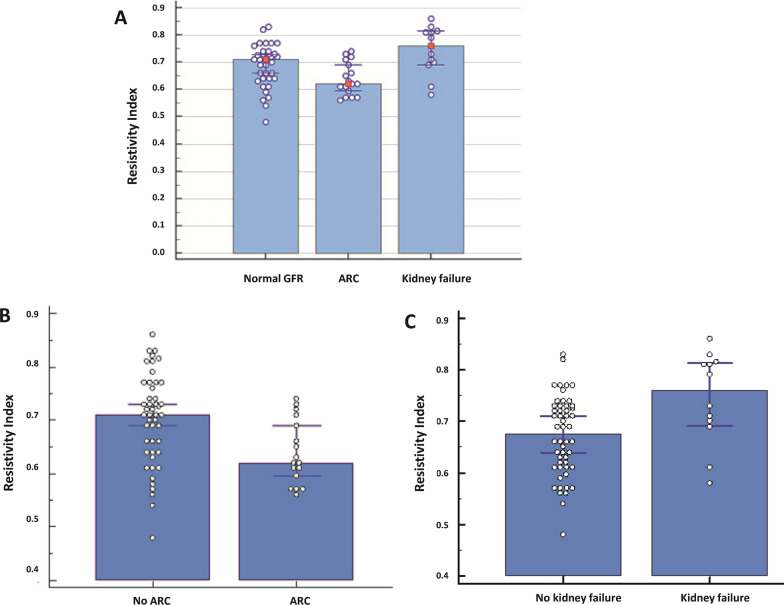
Background: Renal artery Doppler sonography with resistive index (RI) determination is a noninvasive, fast, and reliable diagnostic tool increasingly used in the intensive care unit (ICU) to predict and assess the reversibility of acute kidney injury (AKI). However, interpreting the RI can be challenging due to numerous influencing factors. While some studies have explored various confounding factors, arterial blood gases have received limited attention. Therefore, our study aims to evaluate the impact of arterial blood gases on the RI in the ICU setting.
Methods: This prospective observational study enrolled ICU patients who required blood gas analysis and had not experienced significant hemodynamic changes recently. The RI was measured using standardized Doppler ultrasound within an hour of the arterial blood gases sampling and analysis.
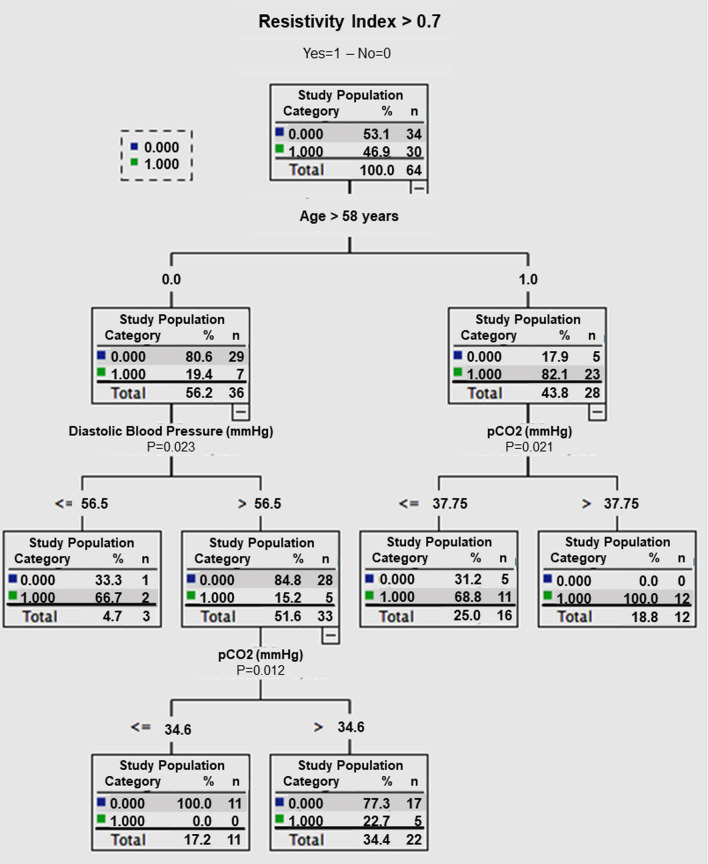
Results: A total of sixty-four patients were included in the analysis. Univariate analysis revealed a correlation between the RI and several variables, including PaCO2 (R = 0.270, p = 0.03), age (R = 0.574, p < 0.0001), diastolic arterial pressure (DAP) (R = - 0.368, p = 0.0028), and SaO2 (R = - 0.284, p = 0.0231). Multivariate analysis confirmed that age > 58 years and PaCO2 were significant factors influencing the RI, with respective odds ratios of 18.67 (p = 0.0003) and 1.132 (p = 0.0267).
Conclusion: The interpretation of renal arterial RI should take into account thresholds for PaCO2, age, and diastolic arterial pressure. Further studies are needed to develop a comprehensive scoring system that incorporates all these cofactors for a reliable analysis of RI levels. Trial registration This observational study, registered under number 70-0914, received approval from local Ethical Committee of Toulouse University Hospital.
Keywords: Acute kidney injury; Arterial blood gases; Intensive care unit; Renal artery Doppler; Resistive index.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
