

Metastasising ameloblastoma or ameloblastic carcinoma? A case report with mutation analyses
- PMID: 37573343
- PMCID: PMC10423427
- DOI: 10.1186/s12903-023-03259-6
Metastasising ameloblastoma or ameloblastic carcinoma? A case report with mutation analyses
Abstract
Background: Ameloblastic carcinoma and metastasising ameloblastoma are rare epithelial odontogenic tumours with aggressive features. Distinguishing between these two lesions is often clinically difficult but necessary to predict tumour behaviour or to plan future therapy. Here, we provide a brief review of the literature available on these two types of lesions and present a new case report of a young man with an ameloblastoma displaying metastatic features. We also use this case to illustrate the similarities and differences between these two types of tumours and the difficulties of their differential diagnosis.
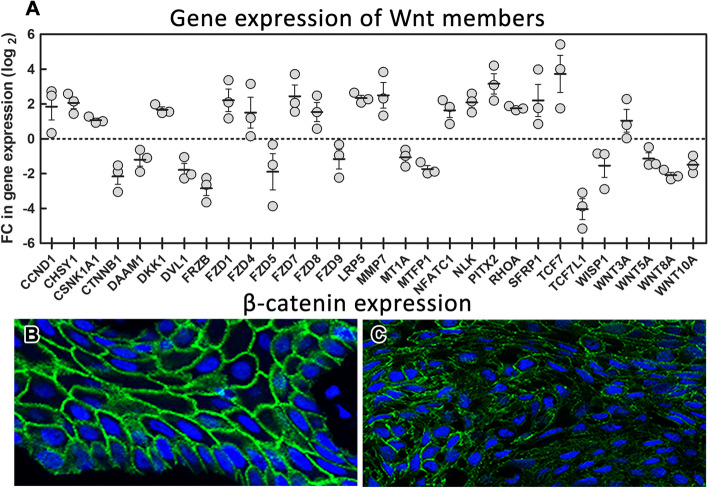
Case presentation: Our histopathological analyses uncovered a metastasising tumour with features of ameloblastic carcinoma, which developed from the ameloblastoma. We profiled the gene expression of Wnt pathway members in ameloblastoma sample of this patient, because multiple molecules of this pathway are involved in the establishing of cell polarity, cell migration or for epithelial-mesenchymal transition during tumour metastasis to evaluate features of tumor behaviour. Indeed, we found upregulation of several cell migration-related genes in our patient. Moreover, we uncovered somatic mutation BRAF p.V600E with known pathological role in cancerogenesis and germline heterozygous FANCA p.S858R mutation, whose interpretation in this context has not been discussed yet.
Conclusions: In conclusion, we have uncovered a unique case of ameloblastic carcinoma associated with an alteration of Wnt signalling and the presence of BRAF mutation. Development of harmful state of our patient might be also supported by the germline mutation in one FANCA allele, however this has to be confirmed by further analyses.
Keywords: Ameloblastoma; BRAF; Benign; Carcinoma; Case report; FANCA; Malignant; Metastasizing; Wnt pathway.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




References
-
- Kramer IR, Pindborg JJ, Shear M. The WHO Histological Typing of Odontogenic Tumours. A commentary on the Second Edition. Cancer. 1992;70(12):2988–94. - PubMed
-
- Palanisamy JC, Jenzer AC. Ameloblastoma. StatPearls. Treasure Island (FL)2022.
-
- Jing W, Xuan M, Lin Y, Wu L, Liu L, Zheng X, et al. Odontogenic tumours: a retrospective study of 1642 cases in a Chinese population. Int J Oral Maxillofac Surg. 2007;36(1):20–25. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
