

Impaired echocardiographic left ventricular global longitudinal strain after pediatric cardiac arrest children is associated with mortality
- PMID: 37574003
- PMCID: PMC10802989
- DOI: 10.1016/j.resuscitation.2023.109936
Impaired echocardiographic left ventricular global longitudinal strain after pediatric cardiac arrest children is associated with mortality
Abstract
Background: Global longitudinal strain (GLS) is an echocardiographic method to identify left ventricular (LV) dysfunction after cardiac arrest that is less sensitive to loading conditions. We aimed to identify the frequency of impaired GLS following pediatric cardiac arrest, and its association with hospital mortality.
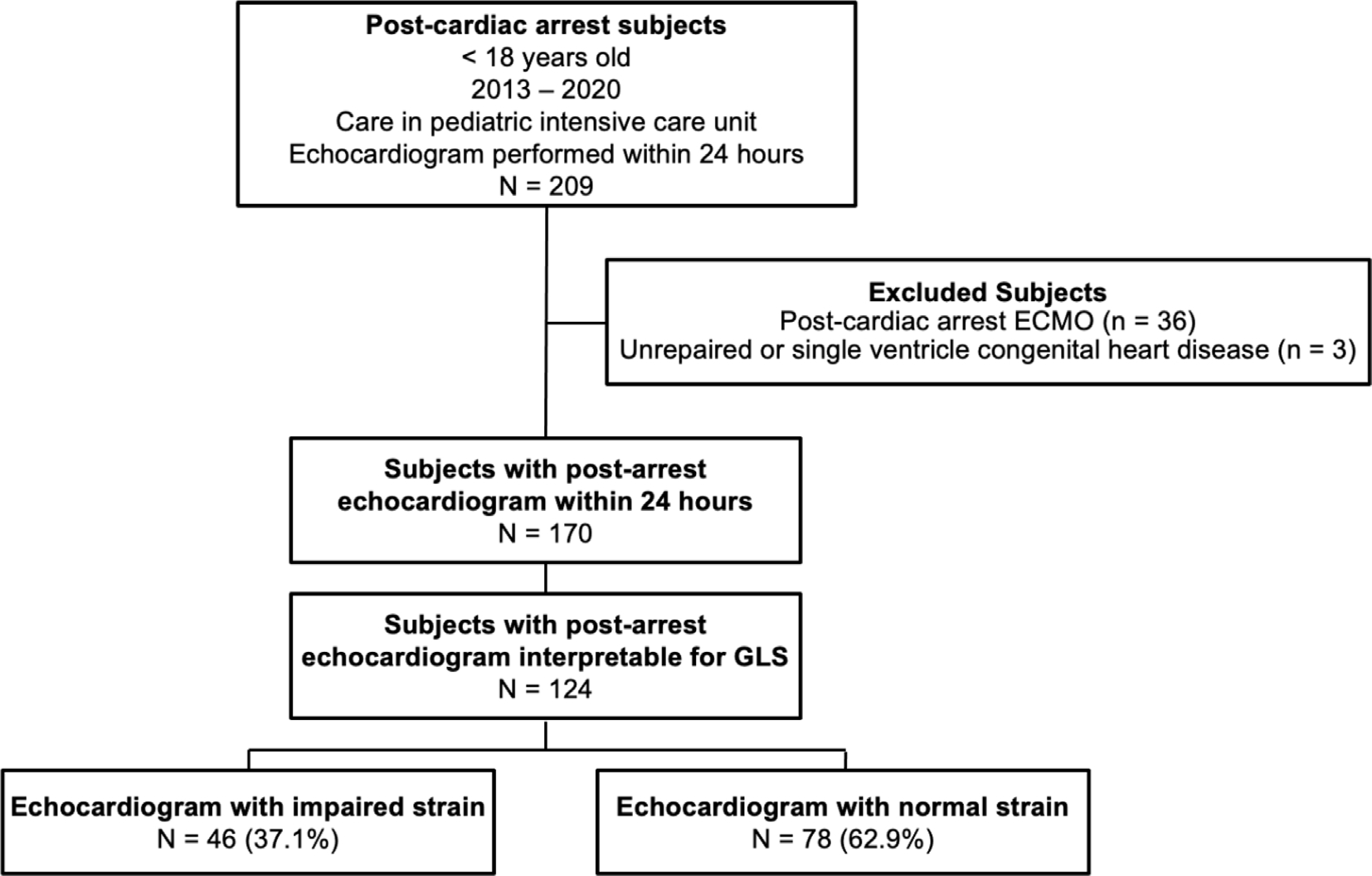
Methods: This is a retrospective single-center cohort study of children <18 years of age treated in the pediatric intensive care unit (PICU) after in- or out-of-hospital cardiac arrest (IHCA and OHCA), with echocardiogram performed within 24 hours of initiation of post-arrest PICU care between 2013 and 2020. Patients with congenital heart disease, post-arrest extracorporeal support, or inability to measure GLS were excluded. Echocardiographic LV ejection fraction (EF) and shortening fraction (SF) were abstracted from the chart. GLS was measured post hoc; impaired strain was defined as LV GLS ≥ 2 SD worse than age-dependent normative values. Demographics and pre-arrest, arrest, and post-arrest characteristics were compared between subjects with normal versus impaired GLS. Correlation between GLS, SF and EF were calculated with Pearson comparison. Logistic regression tested the association of GLS with mortality. Area under the receiver operator curve (AUROC) was calculated for discriminative utility of GLS, EF, and SF with mortality.
Results: GLS was measured in 124 subjects; impaired GLS was present in 46 (37.1%). Subjects with impaired GLS were older (median 7.9 vs. 1.9 years, p < 0.001), more likely to have ventricular tachycardia/fibrillation as initial rhythm (19.6% versus 3.8%, p = 0.017) and had higher peak troponin levels in the first 24 hours post-arrest (median 2.5 vs. 0.5, p = 0.002). There were no differences between arrest location or CPR duration by GLS groups. Subjects with impaired GLS compared to normal GLS had lower median EF (42.6% versus 62.3%) and median SF (23.3% versus 36.6%), all p < 0.001, with strong inverse correlation between GLS and EF (rho -0.76, p < 0.001) and SF (rho -0.71, p < 0.001). Patients with impaired GLS had higher rates of mortality (60% vs. 32%, p = 0.009). GLS was associated with mortality when controlling for age and initial rhythm [aOR 1.17 per 1% increase in GLS (95% CI 1.09-1.26), p < 0.001]. GLS, EF and SF had similar discrimination for mortality: GLS AUROC 0.69 (95% CI 0.60-0.79); EF AUROC 0.71 (95% CI 0.58-0.88); SF AUROC 0.71 (95% CI 0.61-0.82), p = 0.101.
Conclusions: Impaired LV function as measured by GLS after pediatric cardiac arrest is associated with hospital mortality. GLS is a novel complementary metric to traditional post-arrest echocardiography that correlates strongly with EF and SF and is associated with mortality. Future large prospective studies of post-cardiac arrest care should investigate the prognostic utilities of GLS, alongside SF and EF.
Keywords: Cardiac arrest; Mortality; Myocardial dysfunction; Pediatrics; Post-arrest outcomes.
Copyright © 2023 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
