

A Systematic Review and Meta-Analysis on the Efficacy and Safety of Finerenone Therapy in Patients with Cardiovascular and Chronic Kidney Diseases in Type 2 Diabetes Mellitus
- PMID: 37575756
- PMCID: PMC10421409
- DOI: 10.7759/cureus.41746
A Systematic Review and Meta-Analysis on the Efficacy and Safety of Finerenone Therapy in Patients with Cardiovascular and Chronic Kidney Diseases in Type 2 Diabetes Mellitus
Abstract
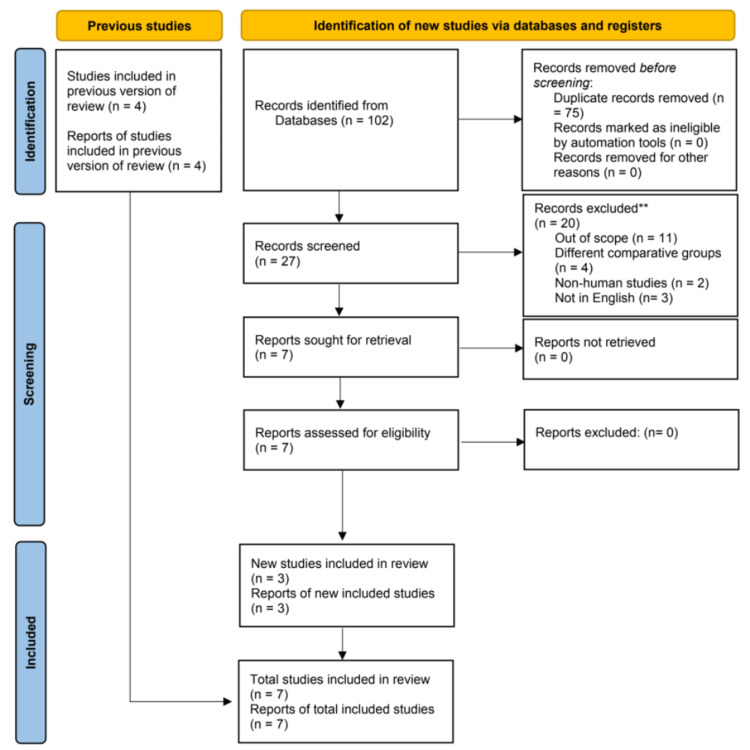
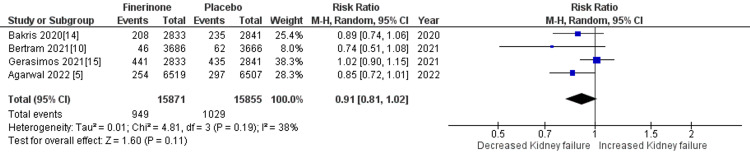
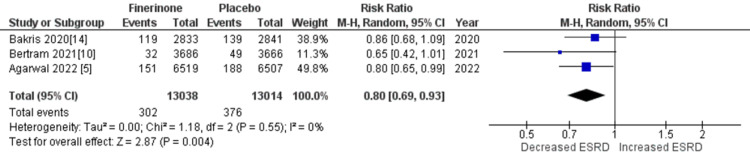
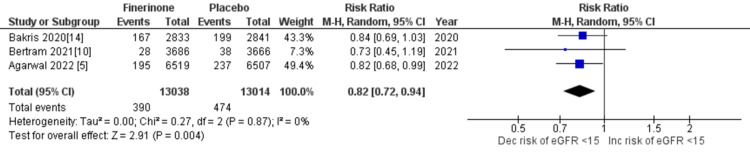
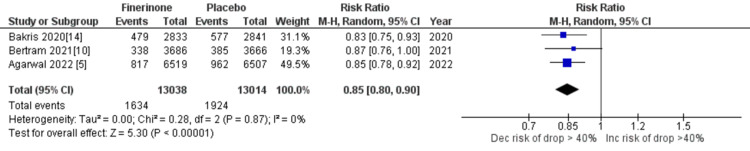
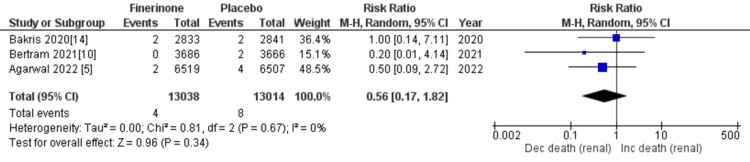
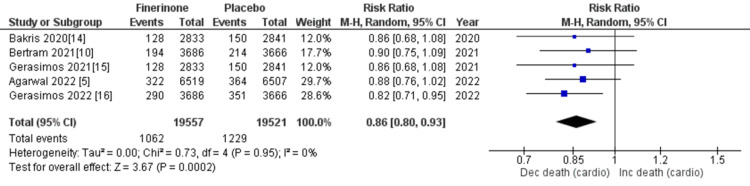
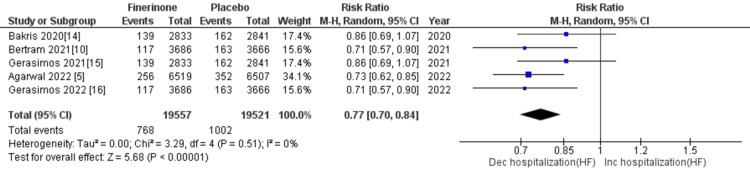
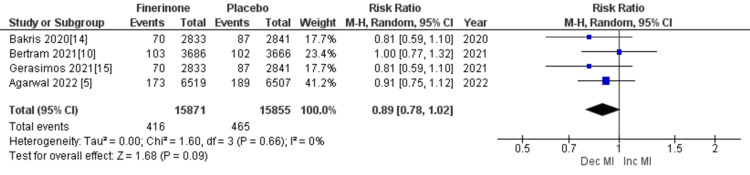
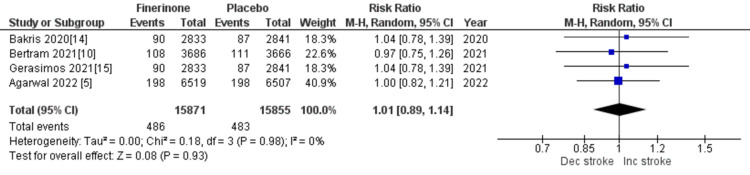
The purpose of this study is to assess the safety and efficacy of finerenone therapy in type 2 diabetes mellitus (T2DM) patients with cardiovascular and chronic renal diseases. This meta-analysis assesses the efficacy and safety of finerenone in the treatment of diabetic kidney disease (DKD). A comprehensive search of PubMed, Embase, and Google Scholar databases was performed to identify relevant randomized controlled trials (RCTs). To quantify the effects of finerenone, the analysis included the estimation of aggregated mean differences (MDs) and relative risks (RRs), as well as 95% confidence intervals (CIs). This meta-analysis included seven double-blind trials with patients suffering from chronic kidney disease (CKD) and T2D. Participants received finerenone or a placebo was assigned at random. The primary efficacy outcomes were cardiovascular mortality, non-fatal myocardial infarction, non-fatal stroke, hospitalization for heart failure, kidney failure, a sustained 57% decrease in the estimated glomerular filtration rate from baseline over four weeks, or renal death. Among the 39,995 patients included in the analysis, finerenone treatment was associated with a lower risk of cardiovascular and renal-related mortality compared to placebo (RR = 0.86 (0.80, 0.93), p = 0.0002; I-squared statistic (I2 ) = 0%) and (RR = 0.56 (0.17, 1.82), p = 0.34; I2 = 0%). In addition, finerenone treatment was associated with a marginally reduced risk of serious adverse events (RR = 0.95 (0.92, 0.97), p = 0.0001; I2 = 0%), although no significant difference in the overall risk of adverse events was observed between the two groups (RR = 1.00 (0.99, 1.01), p = 0.56; I2 = 0%). This study's findings suggest that finerenone administration can reduce the risk of end-stage kidney disease, renal failure, cardiovascular mortality, and hospitalization. Patients with both T2DM and CKD are therefore advised to consider finerenone therapy.
Keywords: cardiovascular disease; chronic kidney disease; ckd; diabetes; finerenone; meta-analysis; non-steroidal mineralocorticoid receptor antagonist.
Copyright © 2023, Jyotsna et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. McDonagh TA, Metra M, Adamo M, et al. Eur Heart J. 2021;42:3599–3726. - PubMed
-
- 2022 aha/acc/hfsa guideline for the management of heart failure: a report of the american college of cardiology/american heart association joint committee on clinical practice guidelines. Heidenreich PA, Bozkurt B, Aguilar D, et al. Circulation. 2022;145:895–1032. - PubMed
-
- Cardiovascular protection with anti-hyperglycemic agents. Deedwania P, Acharya T. Am J Cardiovasc Drugs. 2019;19:249–257. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous