

Systemic Pharmacology Reveals the Potential Targets and Signaling Mechanisms in the Adjuvant Treatment of Brucellosis with Traditional Chinese Medicine
- PMID: 37576692
- PMCID: PMC10413447
- DOI: 10.1021/acsomega.3c03716
Systemic Pharmacology Reveals the Potential Targets and Signaling Mechanisms in the Adjuvant Treatment of Brucellosis with Traditional Chinese Medicine
Abstract
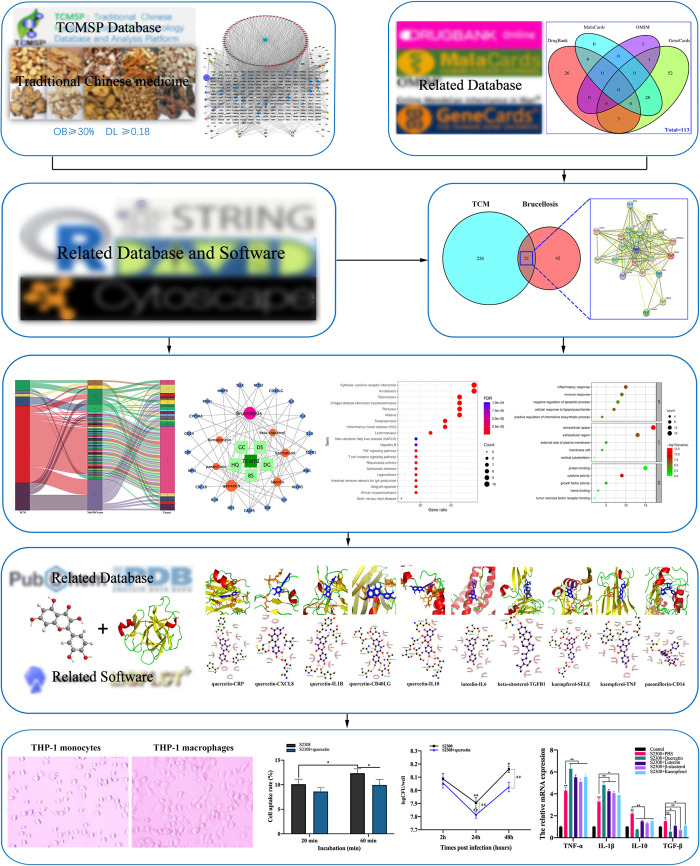
Human brucellosis is one of the world's most common zoonoses, caused by Brucella infection and characterized by induced inflammation, which in severe cases can lead to abortion and sterility in humans and animals. There is growing evidence that traditional Chinese medicine (TCM) is beneficial as an adjunct to the treatment of brucellosis. However, its specific targets of action and molecular mechanisms remain unclear. In this study, a systematic pharmacological approach was applied to demonstrate pharmacological targets, biological functions, and signaling pathways of TCM as an adjunct to the treatment of brucellosis (TCMTB). The results of network pharmacology were further verified by in vitro experiments. Network analysis revealed that 133 active ingredients and 247 targets were screened in TCMTB. Further data analysis identified 21 core targets and 5 core compounds in TCMTB, including beta-sitosterol, quercetin, kaempferol, luteolin, and paeoniflorin. Gene ontology and the Kyoto Encyclopedia of Gene and Genome analysis showed that TCMTB might actively treat brucellosis by regulating inflammatory response, enhancing immune function, and targeting signaling pathways such as tuberculosis and TNF. Molecular docking results showed that multiple compounds could bind to multiple targets. Further, in vitro experiments confirmed that quercetin, among the active compounds screened, induced the strongest immunomodulatory and pro-inflammatory cytokine production during Brucella abortus infection. Further, quercetin induced nitric oxide production, which attenuated the ability of B. abortus to internalize THP-1 cells as well as intracellular survival. This study reveals the mechanism by which TCMTB aids in the treatment of brucellosis through a synergistic multicomponent, multipathway, and multitarget action. The contribution of quercetin treatment to B. abortus infection was demonstrated for the first time, which may be related to the quercetin-induced production of nitric oxide and immunomodulatory and inflammatory cytokines. These predictions of the core compounds and targets may be used in the future for the clinical treatment of brucellosis.
© 2023 The Authors. Published by American Chemical Society.
Conflict of interest statement
The authors declare no competing financial interest.
Figures






References
LinkOut - more resources
Full Text Sources