

Prevalence, definition, and etiology of cesarean scar defect and treatment of cesarean scar disorder: A narrative review
- PMID: 37577060
- PMCID: PMC10412910
- DOI: 10.1002/rmb2.12532
Prevalence, definition, and etiology of cesarean scar defect and treatment of cesarean scar disorder: A narrative review
Abstract
Background: Cesarean scar defects (CSD) are caused by cesarean sections and cause various symptoms. Although there has been no previous consensus on the name of this condition for a long time, it has been named cesarean scar disorder (CSDi).
Methods: This review summarizes the definition, prevalence, and etiology of CSD, as well as the pathophysiology and treatment of CSDi. We focused on surgical therapy and examined the effects and procedures of laparoscopy, hysteroscopy, and transvaginal surgery.
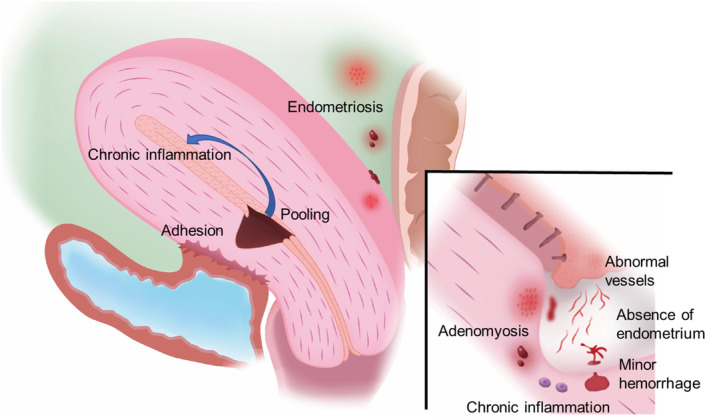
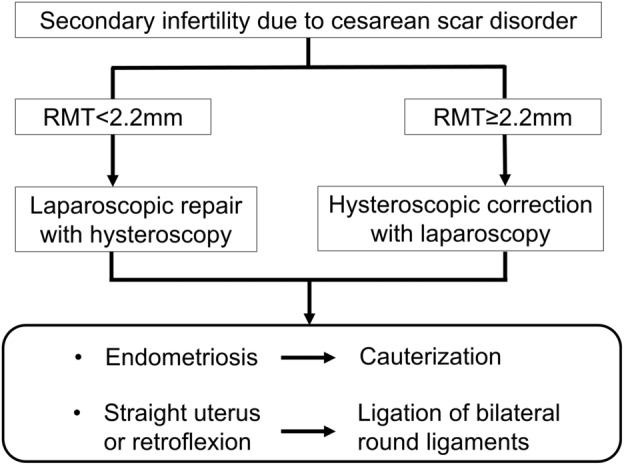
Main findings: The definition of CSD was proposed as an anechoic lesion with a depth of at least 2 mm because of the varied prevalence, owing to the lack of consensus. CSD incidence depends on the number of times, procedure, and situation of cesarean sections. Histopathological findings in CSD are fibrosis and adenomyosis, and chronic inflammation in the uterine and pelvic cavities decreases fertility in women with CSDi. Although the surgical procedures are not standardized, laparoscopic, hysteroscopic, and transvaginal surgeries are effective.
Conclusion: The cause and pathology of CSDi are becoming clear. However, there is variability in the prevalence and treatment strategies. Therefore, it is necessary to conduct further studies using the same definitions.
Keywords: cesarean scar defect; cesarean scar disorder; cesarean section; hysteroscopic surgery; secondary infertility.
© 2023 The Authors. Reproductive Medicine and Biology published by John Wiley & Sons Australia, Ltd on behalf of Japan Society for Reproductive Medicine.
Conflict of interest statement
Takashi Murakami is an Editorial Board member of Reproductive Medicine and Biology and a co‐author of this article. To minimize bias, he was excluded from all editorial decision‐making related to the acceptance of this article for publication.
Figures
References
-
- WHO . WHO statement on caesarean section rates. Reprod Health Matters. 2015;23:149–150. - PubMed
-
- Boerma T, Ronsmans C, Melesse DY, Barros AJD, Barros FC, Juan L, et al. Global epidemiology of use of and disparities in caesarean sections. Lancet. 2018;392:1341–1348. - PubMed
-
- WHO . Caesarean section rates continue to rise, amid growing inequalities in access. Geneva: World Health Organization; 2023.
-
- Maeda E, Ishihara O, Tomio J, Miura H, Kobayashi Y, Terada Y, et al. Cesarean delivery rates for overall and multiple pregnancies in Japan: a descriptive study using nationwide health insurance claims data. J Obstet Gynaecol Res. 2021;47:2099–2109. - PubMed
-
- Erickson SS, Van Voorhis BJ. Intermenstrual bleeding secondary to cesarean scar diverticuli: report of three cases. Obstet Gynecol. 1999;93:802–805. - PubMed
Publication types
LinkOut - more resources
Full Text Sources