

This is a preprint.
Critical Illness Risk and Long-Term Outcomes Following Intensive Care in Pediatric Hematopoietic Cell Transplant Recipients
- PMID: 37577706
- PMCID: PMC10418579
- DOI: 10.1101/2023.07.31.23293444
Critical Illness Risk and Long-Term Outcomes Following Intensive Care in Pediatric Hematopoietic Cell Transplant Recipients
Update in
-
Intensive care risk and long-term outcomes in pediatric allogeneic hematopoietic cell transplant recipients.Blood Adv. 2024 Feb 27;8(4):1002-1017. doi: 10.1182/bloodadvances.2023011002. Blood Adv. 2024. PMID: 38127268 Free PMC article.
Abstract
Background: Allogeneic hematopoietic cell transplantation (HCT) can be complicated by the development of organ toxicity and infection necessitating intensive care. Risk factors for intensive care admission are unclear due to heterogeneity across centers, and long-term outcome data after intensive care are sparse due to a historical paucity of survivors.
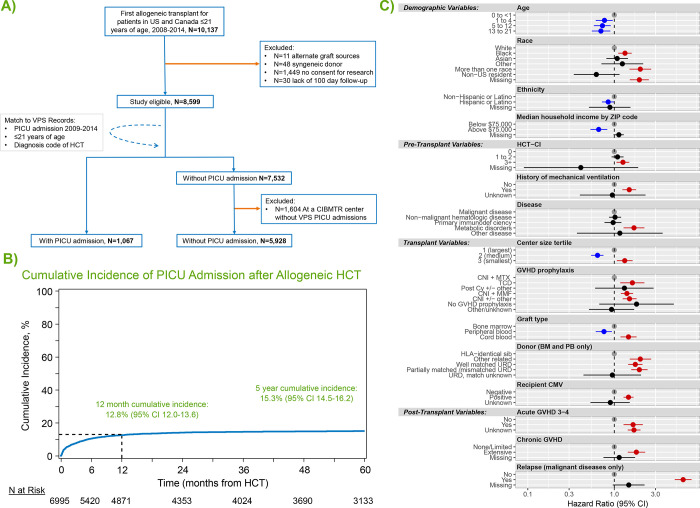
Methods: The Center for International Blood and Marrow Transplant Research (CIBMTR) was queried to identify patients age ≤21 years who underwent a 1st allogeneic HCT between 2008-2014 in the United States or Canada. Records were cross-referenced with the Virtual Pediatric Systems pediatric ICU database to identify intensive care admissions. CIBMTR follow-up data were collected through the year 2020.
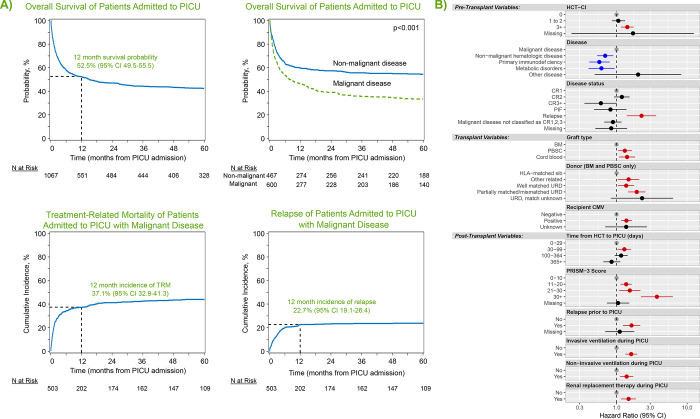
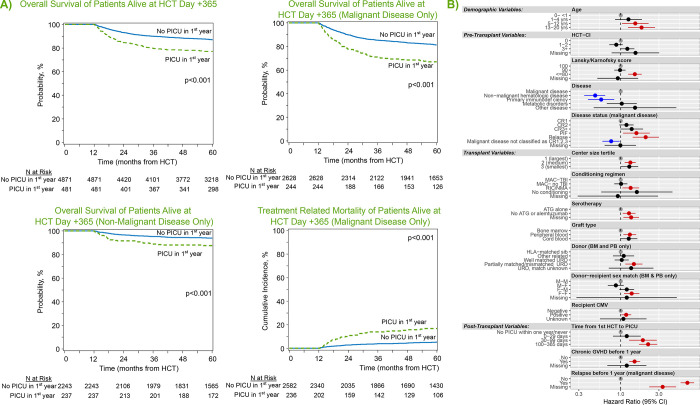
Result: We identified 6,995 pediatric HCT patients from 69 HCT centers, of whom 1,067 required post-HCT intensive care. The cumulative incidence of PICU admission was 8.3% at day +100, 12.8% at 1 year, and 15.3% at 5 years post HCT. PICU admission was linked to younger age, lower median zip code income, Black or multiracial background, pre-transplant organ toxicity, pre-transplant CMV seropositivity, use of umbilical cord blood and/or HLA-mismatched allografts, and the development of post-HCT graft-versus-host disease or malignancy relapse. Among PICU patients, survival to ICU discharge was 85.7% but more than half of ICU survivors were readmitted to a PICU during the study interval. Overall survival from the time of 1st PICU admission was 52.5% at 1 year and 42.6% at 5 years. Long-term post-ICU survival was worse among patients with malignant disease (particularly if relapsed), as well as those with poor pre-transplant organ function and alloreactivity risk-factors. In a landmark analysis of all 1-year HCT survivors, those who required intensive care in the first year had 10% lower survival at 5 years (77.1% vs. 87.0%, p<0.001) and developed new dialysis-dependent renal failure at a greater rate (p<0.001).
Conclusions: Intensive care management is common in pediatric HCT patients. Survival to ICU discharge is high, but ongoing complications necessitate recurrent ICU admission and lead to a poor 1-year outcome in many patients. Together, these data suggest an ongoing burden of toxicity in pediatric HCT patients that continues to limit long-term survival.
Figures
References
-
- D’Souza A, Fretham C, Lee SJ, Aurora M, Brunner J, Chhabra S, Devine S, Eapen M, Hamadani M, Hari P, Pasquini MC, Phelan RA, Riches ML, Rizzo JD, Saber W, Shaw BE, Spellman SR, Steinert P, Weisdorf DJ, Horowitz MM. Current Use and Trends in Hematopoietic Cell Transplantation in the United States. Biol Blood Marrow Transplant. Elsevier; 2020;26(8):e177–182. - PMC - PubMed
-
- Broglie L, Fretham C, Al-Seraihy A, George B, Kurtzberg J, Loren A, MacMillan M, Martinez C, Davies SM, Pasquini MC. Pulmonary Complications in Pediatric and Adolescent Patients Following Allogeneic Hematopoietic Cell Transplantation. Biol Blood Marrow Transplant J Am Soc Blood Marrow Transplant. 2019. Oct;25(10):2024–2030. - PMC - PubMed
-
- Kaya Z, Weiner DJ, Yilmaz D, Rowan J, Goyal RK. Lung function, pulmonary complications, and mortality after allogeneic blood and marrow transplantation in children. Biol Blood Marrow Transplant J Am Soc Blood Marrow Transplant. United States; 2009;15(7):817–826. - PubMed
-
- Zinter MS, Logan BR, Fretham C, Sapru A, Abraham A, Aljurf MD, Arnold SD, Artz A, Auletta JJ, Chhabra S, Copelan E, Duncan C, Gale RP, Guinan E, Hematti P, Keating AK, Marks DI, Olsson R, Savani BN, Ustun C, Williams KM, Pasquini MC, Dvorak CC. Comprehensive Prognostication in Critically Ill Pediatric Hematopoietic Cell Transplant Patients: Results from Merging the Center for International Blood and Marrow Transplant Research (CIBMTR) and Virtual Pediatric Systems (VPS) Registries. Biol Blood Marrow Transplant J Am Soc Blood Marrow Transplant. United States: . Published by Elsevier Inc; 2020;26(2):333–342. - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials