

Hepatic arterial infusion chemotherapy versus transarterial chemoembolization, potential conversion therapies for single huge hepatocellular carcinoma: a retrospective comparison study
- PMID: 37578432
- PMCID: PMC10651280
- DOI: 10.1097/JS9.0000000000000654
Hepatic arterial infusion chemotherapy versus transarterial chemoembolization, potential conversion therapies for single huge hepatocellular carcinoma: a retrospective comparison study
Abstract
Background: The treatment efficacy of transarterial chemoembolization (TACE) and hepatic arterial infusion chemotherapy (HAIC) for huge single hepatocellular carcinoma (HCC) has not been fully documented. The aim of this study was to compare TACE and HAIC for patients with solitary nodular HCCs greater than or equal to 10 cm without vascular invasion and metastasis.
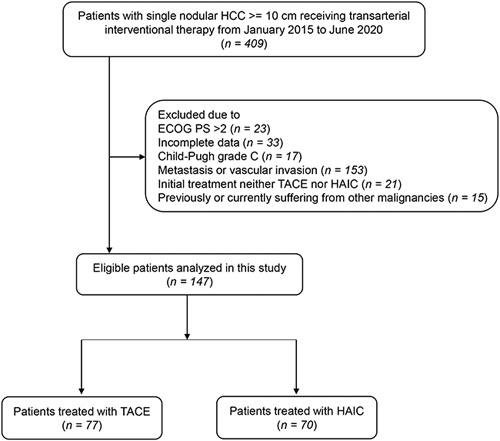
Methods: From July 2015 to June 2020, a total of 147 patients with single nodular HCC greater than or equal to 10 cm without vascular invasion and metastasis receiving TACE ( n =77) or HAIC ( n =70) were retrospectively enrolled. The tumor response, overall survival (OS), and progression-free survival (PFS) were investigated and compared. The treatment outcome of two transarterial interventional therapies was explored.
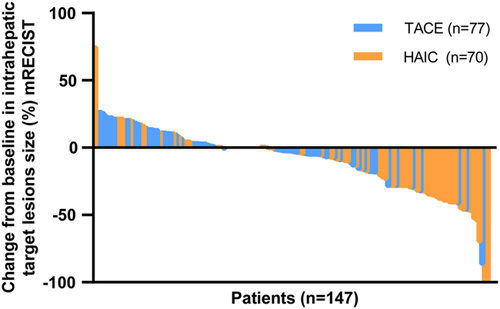
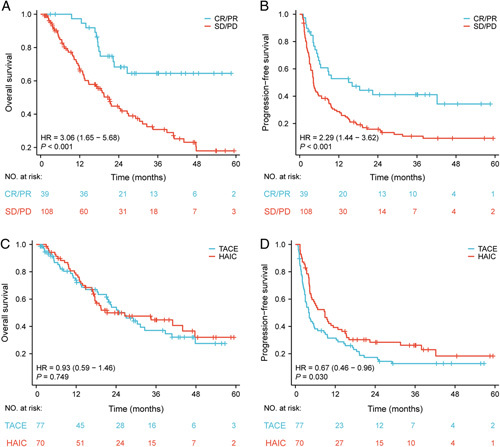
Results: The objective response rate and PFS were higher in patients who received HAIC than in those who received TACE (44.3 vs. 10.4% and 8.9 vs. 4.2 months, respectively; P =0.001 and P =0.030), whereas the disease control rate and OS were not significantly different (92.9 vs. 84.4% and 21.3 vs. 26.6 months, respectively; P =0.798 and P =0.749). The decreased levels of alpha-fetoprotein and protein induced by vitamin K absence or antagonist-II (PIVKA-II) in patients treated with HAIC were significantly higher than those treated with TACE ( P =0.038 and P <0.001). Multivariable analysis showed that the aspartate aminotransferase/platelet ratio index was associated with OS, whereas albumin-bilirubin grade and PIVKA-II were associated with PFS.
Conclusions: HAIC has better potential than TACE to control local tumors for huge single HCC without vascular invasion and metastasis and thus may be the preferred conversion therapy for these tumors.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- Villanueva A. Hepatocellular Carcinoma, eng. New Eng J Med 2019;380:1450–1462. - PubMed
-
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma, eng. Lancet (London, England) 2018;391:1301–1314. - PubMed
-
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol 2018;69:182–236. - PubMed
-
- Yau T, Tang VY, Yao TJ, et al. Development of Hong Kong Liver Cancer staging system with treatment stratification for patients with hepatocellular carcinoma. Gastroenterology 2014;146:1691–700 e3. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
