

IPX203 vs Immediate-Release Carbidopa-Levodopa for the Treatment of Motor Fluctuations in Parkinson Disease: The RISE-PD Randomized Clinical Trial
- PMID: 37578800
- PMCID: PMC10425876
- DOI: 10.1001/jamaneurol.2023.2679
IPX203 vs Immediate-Release Carbidopa-Levodopa for the Treatment of Motor Fluctuations in Parkinson Disease: The RISE-PD Randomized Clinical Trial
Abstract
Importance: Levodopa has a short half-life and a limited window of opportunity for absorption in the proximal small intestine. IPX203 is an oral, extended-release formulation of carbidopa-levodopa developed to address these limitations.
Objective: To assess the efficacy and safety of IPX203 vs immediate-release carbidopa-levodopa in patients with Parkinson disease who are experiencing motor fluctuations.
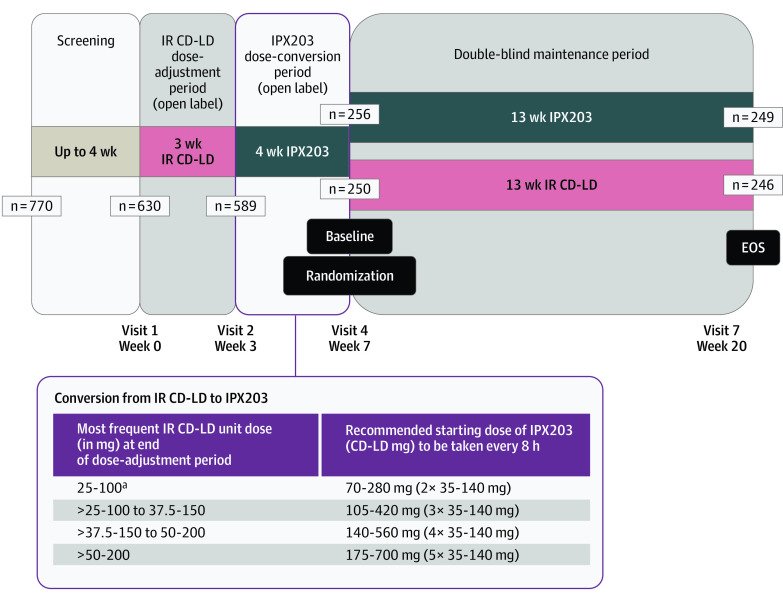
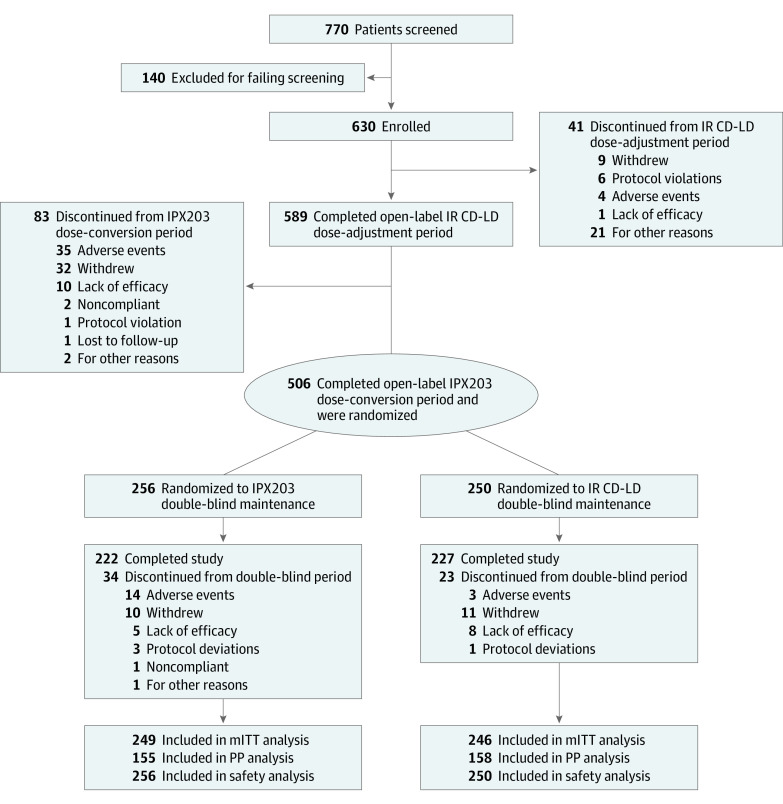
Design, setting, and participants: RISE-PD was a 20-week, randomized, double-blind, double-dummy, active-controlled, phase 3 clinical trial. The study was conducted between November 6, 2018, and June 15, 2021, at 105 academic and clinical centers in the US and Europe. Patients with Parkinson disease taking a total daily dose of 400 mg or more of levodopa and experiencing an average of 2.5 hours or more daily off-time were included in the study. A total of 770 patients were screened, 140 were excluded (those taking controlled-release carbidopa-levodopa apart from a single daily bedtime dose, Rytary (Amneal Pharmaceuticals), additional carbidopa or benserazide, or catechol O-methyl transferase inhibitors or who had a history of psychosis within the past 10 years), and 630 were enrolled in the trial.
Interventions: Following open-label immediate-release carbidopa-levodopa dose adjustment (3 weeks) and conversion to IPX203 (4 weeks), patients were randomized in a 1:1 ratio to double-blind, double-dummy treatment with immediate-release carbidopa-levodopa or IPX203 for 13 weeks.
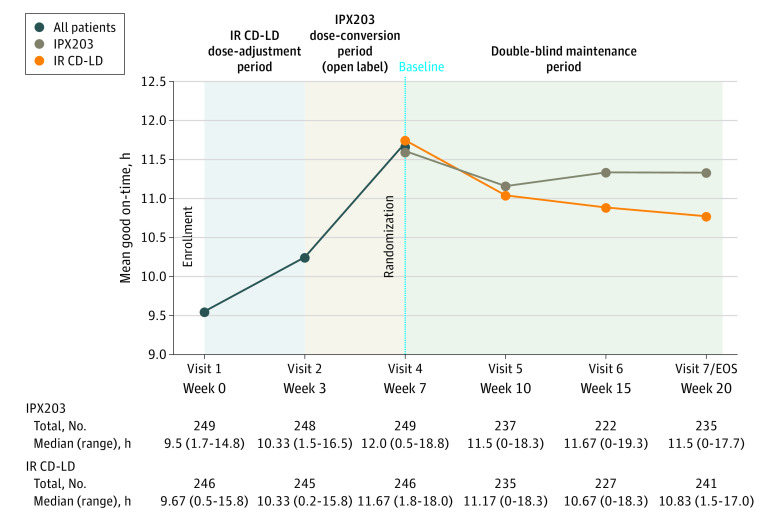
Main outcome and measures: The primary end point was mean change in daily good on-time (ie, on-time without troublesome dyskinesia) from baseline to the end of the double-blind treatment period.
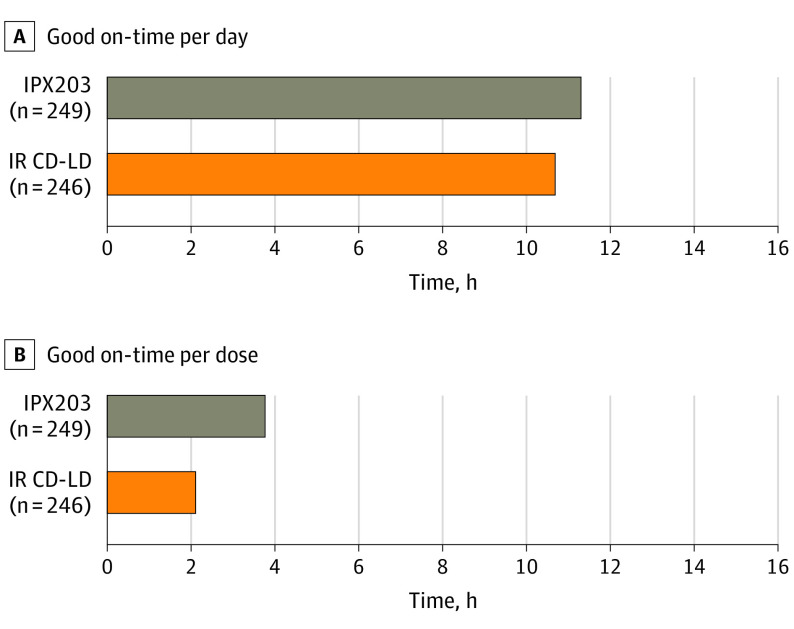
Results: A total of 630 patients (mean [SD] age, 66.5 [8.95] years; 396 [62.9%] men) were enrolled, and 506 patients were randomly assigned to receive IPX203 (n = 256) or immediate-release carbidopa-levodopa (n = 250). The study met its primary end point, demonstrating statistically significant improvement in daily good on-time for IPX203 compared to immediate-release carbidopa-levodopa (least squares mean, 0.53 hours; 95% CI, 0.09-0.97; P = .02), with IPX203 dosed a mean 3 times per day vs 5 times per day for immediate-release carbidopa-levodopa. Good on-time per dose increased by 1.55 hours with IPX203 compared to immediate-release carbidopa-levodopa (95% CI, 1.37-1.73; P < .001). IPX203 was well tolerated. The most common adverse events in the double-blind phase (IPX203 vs immediate-release carbidopa-levodopa) were nausea (4.3% vs 0.8%) and anxiety (2.7% vs 0.0%).
Conclusions and relevance: In this study, IPX203 provided more hours of good on-time per day than immediate-release carbidopa-levodopa, even as IPX203 was dosed less frequently.
Trial registration: ClinicalTrials.gov Identifier: NCT03670953.
Conflict of interest statement
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
