

Viral burden is associated with age, vaccination, and viral variant in a population-representative study of SARS-CoV-2 that accounts for time-since-infection-related sampling bias
- PMID: 37578971
- PMCID: PMC10449197
- DOI: 10.1371/journal.ppat.1011461
Viral burden is associated with age, vaccination, and viral variant in a population-representative study of SARS-CoV-2 that accounts for time-since-infection-related sampling bias
Erratum in
-
Correction: Viral burden is associated with age, vaccination, and viral variant in a population-representative study of SARS-CoV-2 that accounts for time-since-infection-related sampling bias.PLoS Pathog. 2023 Oct 6;19(10):e1011706. doi: 10.1371/journal.ppat.1011706. eCollection 2023 Oct. PLoS Pathog. 2023. PMID: 37801435 Free PMC article.
Abstract
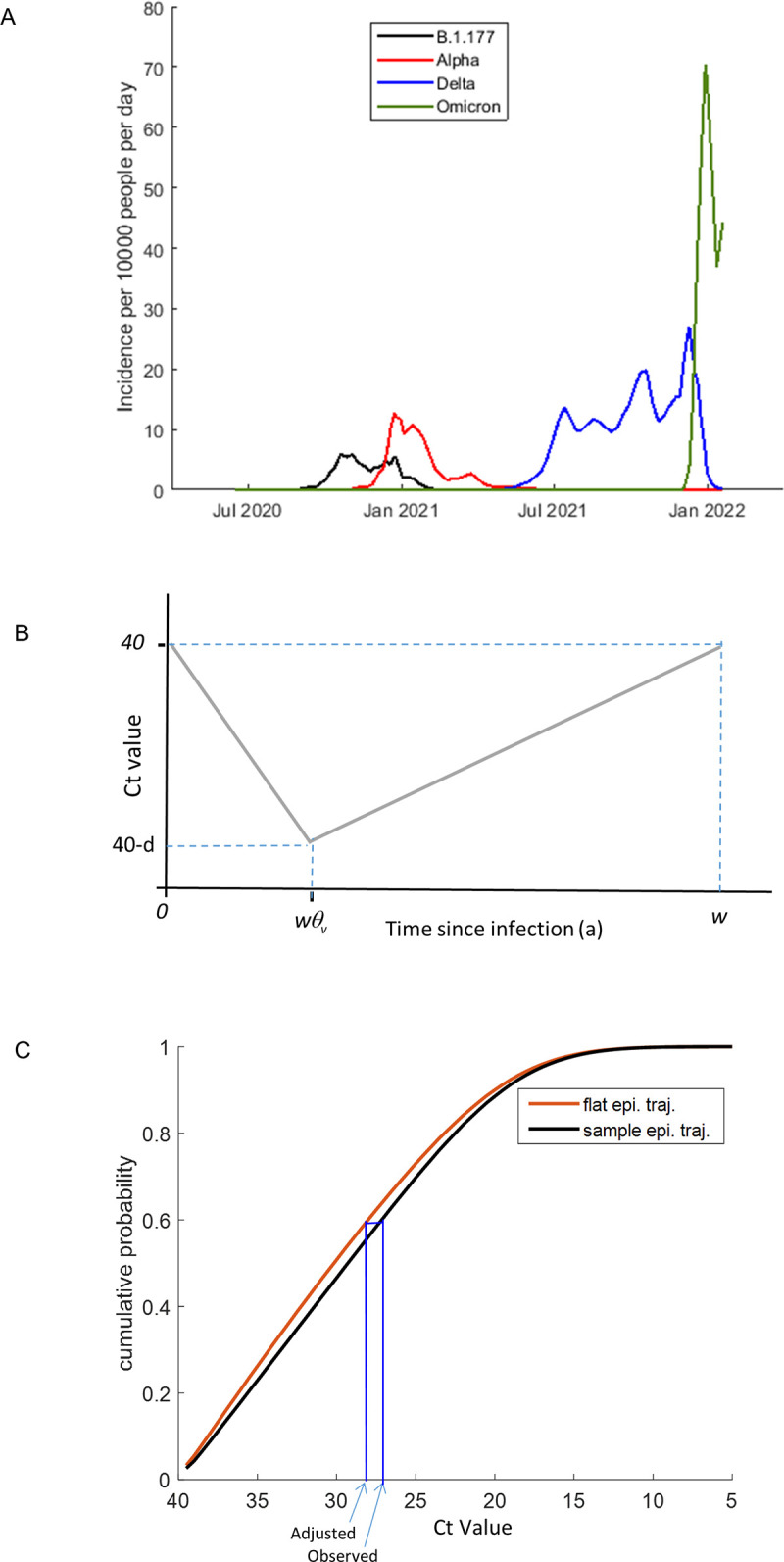
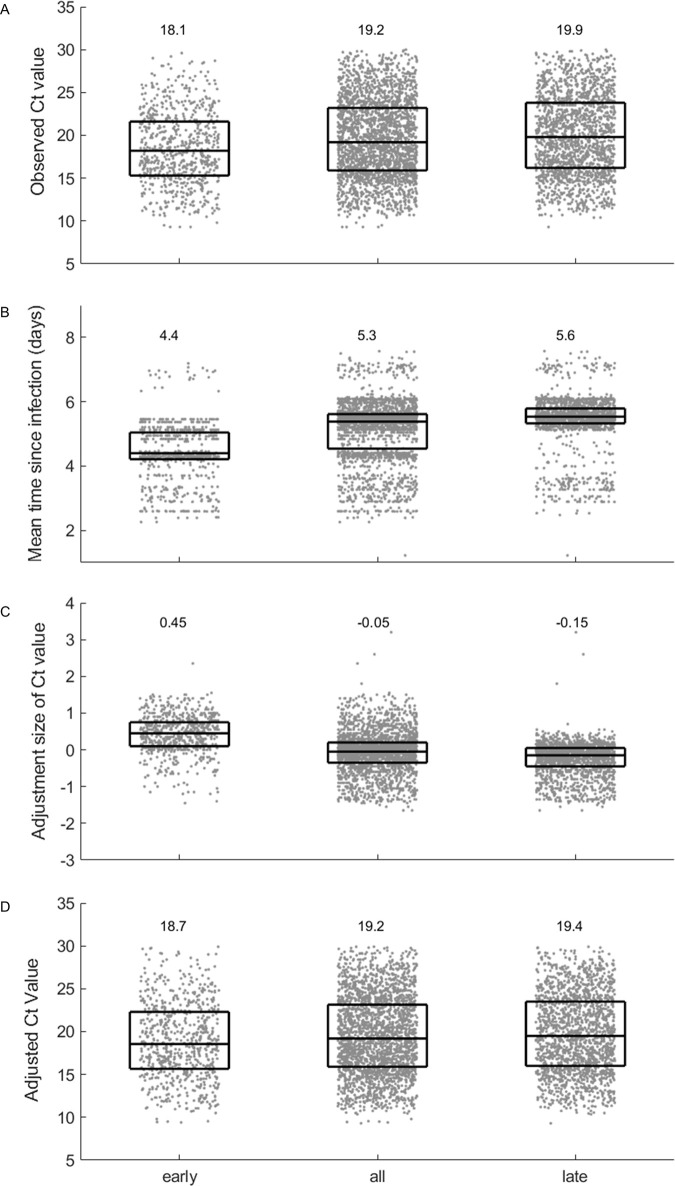
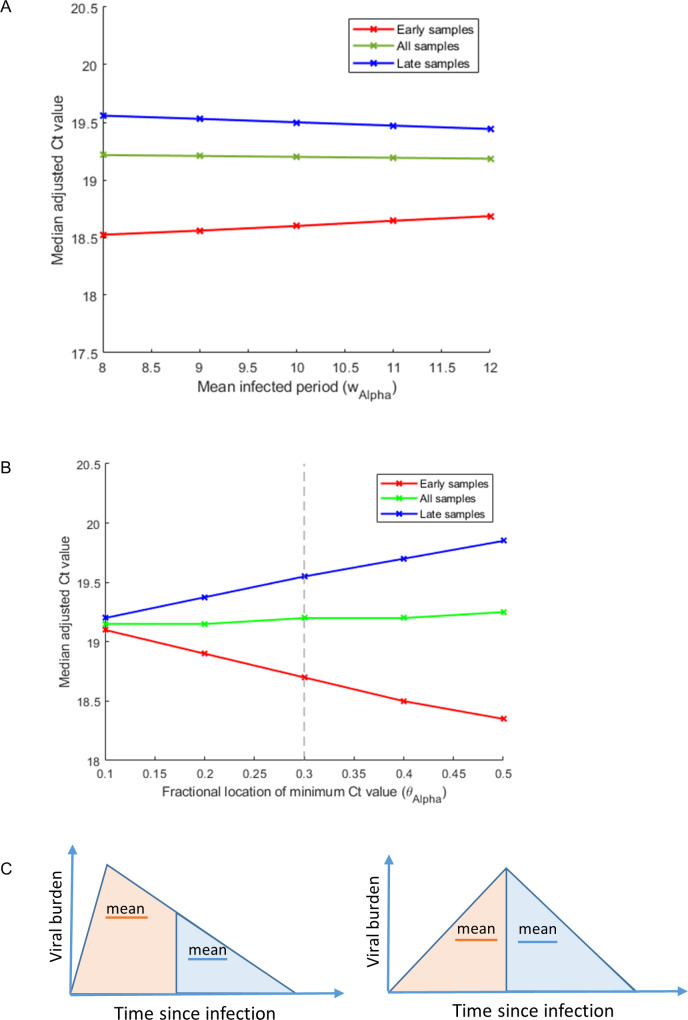
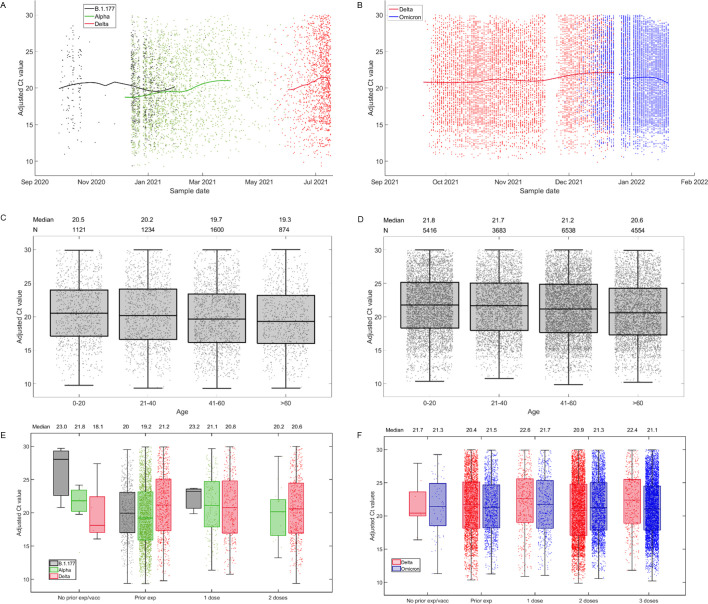
In this study, we evaluated the impact of viral variant, in addition to other variables, on within-host viral burden, by analysing cycle threshold (Ct) values derived from nose and throat swabs, collected as part of the UK COVID-19 Infection Survey. Because viral burden distributions determined from community survey data can be biased due to the impact of variant epidemiology on the time-since-infection of samples, we developed a method to explicitly adjust observed Ct value distributions to account for the expected bias. By analysing the adjusted Ct values using partial least squares regression, we found that among unvaccinated individuals with no known prior exposure, viral burden was 44% lower among Alpha variant infections, compared to those with the predecessor strain, B.1.177. Vaccination reduced viral burden by 67%, and among vaccinated individuals, viral burden was 286% higher among Delta variant, compared to Alpha variant, infections. In addition, viral burden increased by 17% for every 10-year age increment of the infected individual. In summary, within-host viral burden increases with age, is reduced by vaccination, and is influenced by the interplay of vaccination status and viral variant.
Copyright: © 2023 Fryer et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Allen H, Vusirikala A, Flannagan J, Twohig KA, Zaidi A, Chudasama D, et al.. Household transmission of COVID-19 cases associated with SARS-CoV-2 delta variant (B.1.617.2): national case-control study. Lancet Reg Health Eur. 2022;12:100252. Epub 2021/11/04. doi: 10.1016/j.lanepe.2021.100252 ; PubMed Central PMCID: PMC8552812. - DOI - PMC - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
