

Disease severity and mortality in Alzheimer's disease: an analysis using the U.S. National Alzheimer's Coordinating Center Uniform Data Set
- PMID: 37580727
- PMCID: PMC10424331
- DOI: 10.1186/s12883-023-03353-w
Disease severity and mortality in Alzheimer's disease: an analysis using the U.S. National Alzheimer's Coordinating Center Uniform Data Set
Abstract
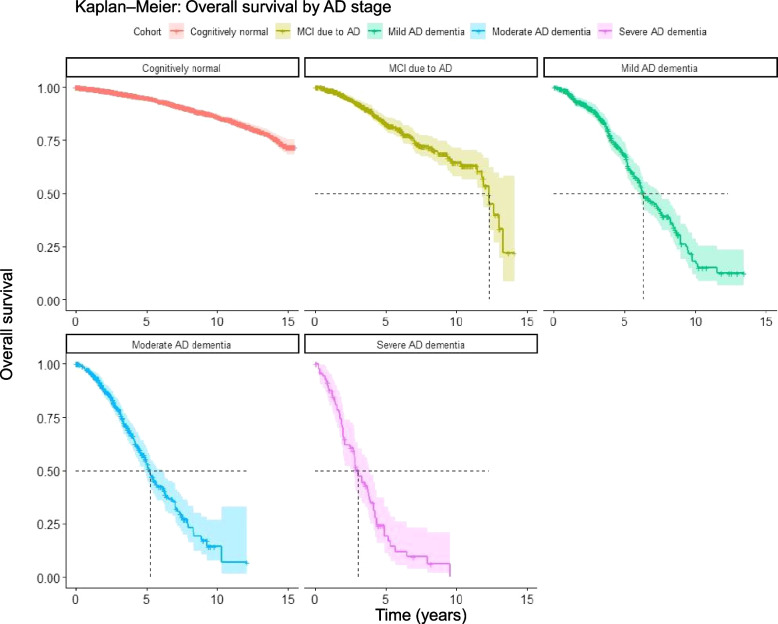
Background: Evidence on the relative risk of death across all stages of Alzheimer's disease (AD) is lacking but greatly needed for the evaluation of new interventions. We used data from the Uniform Data Set (UDS) of the National Alzheimer's Coordinating Center (NACC) to assess the expected survival of a person progressing to a particular stage of AD and the relative risk of death for a person in a particular stage of AD compared with cognitively normal (CN) people.
Methods: This was a retrospective observational cohort study of mortality and its determinants in participants with incident mild cognitive impairment (MCI) due to AD or AD dementia compared with CN participants. Overall survival and hazard ratios of all-cause mortality in participants ≥ 50 years of age with clinically assessed or diagnosed MCI due to AD, or mild, moderate, or severe AD dementia, confirmed by Clinical Dementia Rating scores, versus CN participants were estimated, using NACC UDS data. Participants were followed until death, censoring, or until information to determine disease stage was missing.
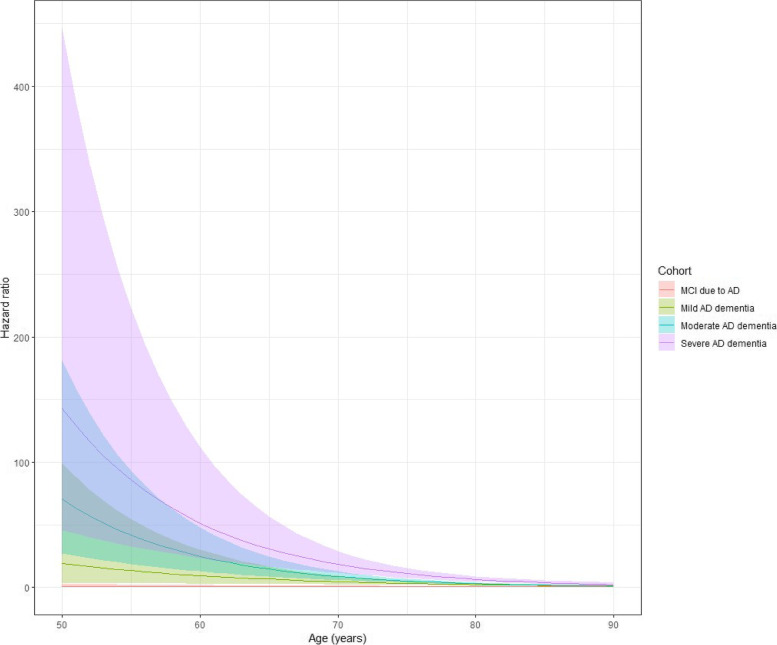
Results: Aged between 50 and 104 years, 12,414 participants met the eligibility criteria for the study. Participants progressing to MCI due to AD or AD dementia survived a median of 3-12 years, with higher mortality observed in more severe stages. Risk of death increased with the severity of AD dementia, with the increase significantly higher at younger ages. Participants with MCI due to AD and CN participants had a similar risk of death after controlling for confounding factors.
Conclusions: Relative all-cause mortality risk increases with AD severity, more so at younger ages. Mortality does not seem to be higher for those remaining in MCI due to AD. Findings might imply potential benefit of lower mortality if preventing or delaying the progression of AD is successful, and importantly, this potential benefit might be greater in relatively younger people. Future research should replicate our study in other samples more representative of the general US population as well as other populations around the world.
Keywords: Alzheimer; Comorbidity; Institution; Mild cognitive impairment; Mortality; Predementia; Prodromal AD.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
VC, SG, and AR are employees and shareholders of F. Hoffmann-La Roche Ltd. SG is a shareholder of Novartis AG. SZ is employed by Genesis Research, the recipient of consulting fees from F. Hoffmann-La Roche Ltd. MV has received research funding from F. Hoffmann-La Roche Ltd and Biogen in past and consults for F. Hoffmann-La Roche Ltd; she receives research funding from NIH and has equity ownership in Abbott Laboratories, Johnson & Johnson, Medtronic, Merck, and Amgen. AG is a partner of Quantify Research, providing consultancy services to pharmaceutical companies, as well as other private and public organizations and institutions.
Figures
References
-
- Gustavsson A, Norton N, Fast T, Frolich L, Georges J, et al. Global estimates on the number of persons across the Alzheimer's disease continuum. Alzheimers Dement. 2023;19:658–70. - PubMed
-
- Gustavsson A, Raket LL, Lilja M, Rutten-Jacobs L, Fues Wahl H, et al. Health utility in preclinical and prodromal Alzheimer's disease for establishing the value of new disease-modifying treatments-EQ-5D data from the Swedish BioFINDER study. Alzheimers Dement. 2021;17:1832–42. - PubMed
-
- WHO. Global status report on the public health response to dementia. Geneva: World Health Organization,. 2021.
Publication types
MeSH terms
Grants and funding
- P50 AG005142/AG/NIA NIH HHS/United States
- P50 AG016573/AG/NIA NIH HHS/United States
- P50 AG047266/AG/NIA NIH HHS/United States
- P30 AG010161/AG/NIA NIH HHS/United States
- P50 AG025688/AG/NIA NIH HHS/United States
- P50 AG005133/AG/NIA NIH HHS/United States
- P20 AG068077/AG/NIA NIH HHS/United States
- P30 AG072977/AG/NIA NIH HHS/United States
- P30 AG010129/AG/NIA NIH HHS/United States
- P50 AG033514/AG/NIA NIH HHS/United States
- P30 AG013854/AG/NIA NIH HHS/United States
- P30 AG053760/AG/NIA NIH HHS/United States
- P20 AG068082/AG/NIA NIH HHS/United States
- P30 AG010124/AG/NIA NIH HHS/United States
- P50 AG023501/AG/NIA NIH HHS/United States
- P20 AG068053/AG/NIA NIH HHS/United States
- P50 AG005131/AG/NIA NIH HHS/United States
- P30 AG010133/AG/NIA NIH HHS/United States
- P50 AG016574/AG/NIA NIH HHS/United States
- P50 AG005146/AG/NIA NIH HHS/United States
- U24 AG072122/AG/NIA NIH HHS/United States
- P30 AG035982/AG/NIA NIH HHS/United States
- P50 AG008702/AG/NIA NIH HHS/United States
- P30 AG008051/AG/NIA NIH HHS/United States
- P50 AG005681/AG/NIA NIH HHS/United States
- P30 AG013846/AG/NIA NIH HHS/United States
- P50 AG047270/AG/NIA NIH HHS/United States
- P50 AG005136/AG/NIA NIH HHS/United States
- P30 AG049638/AG/NIA NIH HHS/United States
- P30 AG012300/AG/NIA NIH HHS/United States
- P50 AG005134/AG/NIA NIH HHS/United States
- P30 AG008017/AG/NIA NIH HHS/United States
- P30 AG066546/AG/NIA NIH HHS/United States
- P50 AG005138/AG/NIA NIH HHS/United States
- P50 AG047366/AG/NIA NIH HHS/United States
- P20 AG068024/AG/NIA NIH HHS/United States
- P30 AG072958/AG/NIA NIH HHS/United States
- P30 AG019610/AG/NIA NIH HHS/United States
- P30 AG072947/AG/NIA NIH HHS/United States
- P30 AG072959/AG/NIA NIH HHS/United States
- P30 AG028383/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
