

Risk Factors and Causes of Reoperation in Lumbar Disc Herniation Patients after Percutaneous Endoscopic Lumbar Discectomy: A Retrospective Case Series with a Minimum 2-Year Follow-Up
- PMID: 37580900
- PMCID: PMC10439676
- DOI: 10.12659/MSM.939844
Risk Factors and Causes of Reoperation in Lumbar Disc Herniation Patients after Percutaneous Endoscopic Lumbar Discectomy: A Retrospective Case Series with a Minimum 2-Year Follow-Up
Abstract
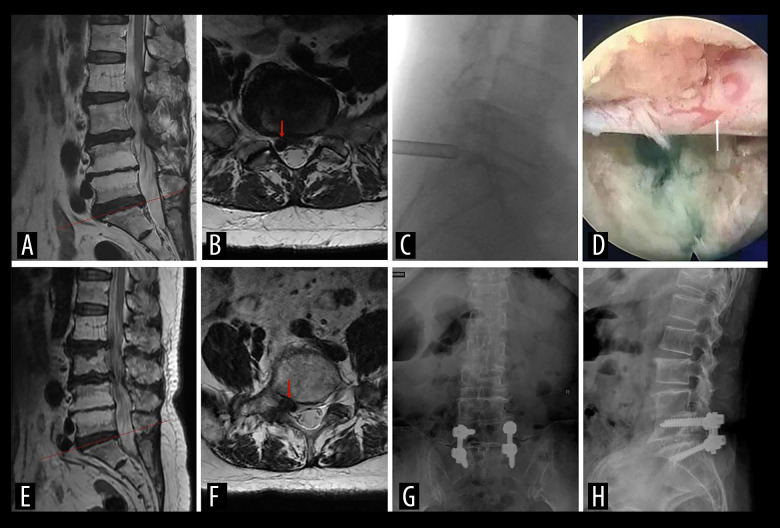
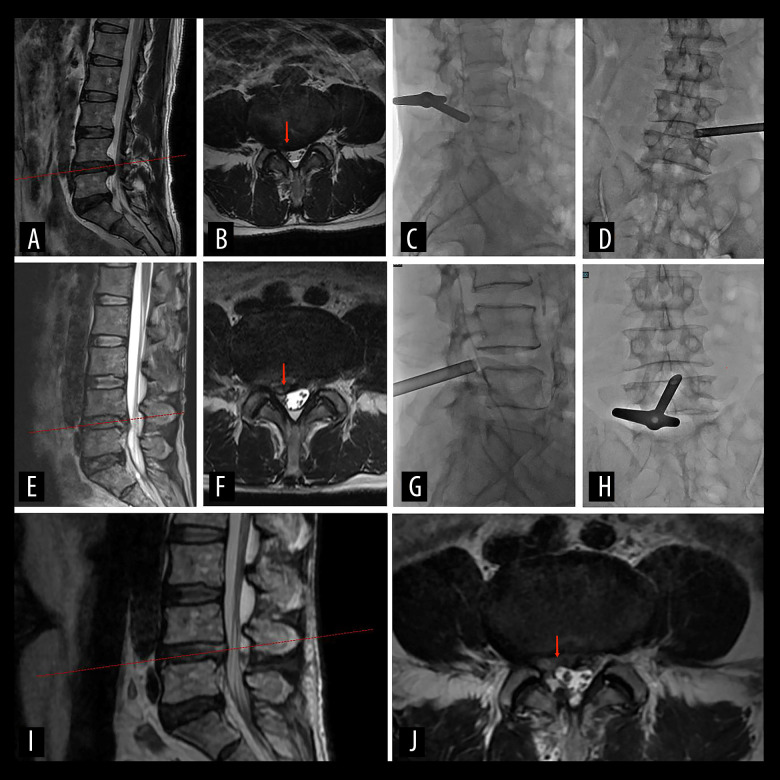
BACKGROUND Percutaneous endoscopic lumbar discectomy (PELD) has gained popularity as a minimally invasive surgery for treating lumbar disc herniation. However, there is limited research focusing on the reoperation rate and its associated factors. This study aims to investigate the rate of reoperation and identify the causes and risk factors for reoperation after PELD. MATERIAL AND METHODS We conducted a retrospective analysis of patients who underwent PELD (interlaminar and transforaminal approaches) at our hospital from November 2016 to May 2020. A matched case-control design was employed to identify relevant risk factors for reoperation, with a matching ratio of 1:3. Clinical characteristics and radiological parameters were compared, and univariate analysis was performed using independent samples t-test and chi-squared test. RESULTS Among the 435 patients included in the study, the reoperation rate for those with a minimum 2-year follow-up was 6.2% (27/435). The causes of reoperation and their respective rates were as follows: recurrence of lumbar disc herniation (3.2%, 14/435), incomplete decompression (1.8%, 8/435), persistent low back pain (0.7%, 3/435), and postoperative infection (0.5%, 2/435). Univariate analysis revealed that age (P=0.015), Pfirrmann grade IV-V (P=0.017), and lack of active straight leg raise exercises (P=0.026) were significantly associated with reoperation. Multiple logistic regression analysis indicated that age (P=0.001), Pfirrmann grade IV-V (P=0.033), and lack of active straight leg raise exercises postoperatively (P=0.003) were independent risk factors for reoperation after PELD. CONCLUSIONS The primary cause of reoperation in lumbar disc herniation patients after PELD was recurrence of the herniation. Additionally, severe disc degeneration, older age, and lack of active straight leg raise exercises were identified as significant risk factors associated with an increased reoperation rate.
Conflict of interest statement
Figures



Similar articles
-
Percutaneous Endoscopic Lumbar Discectomy via Transforaminal Approach Combined with Interlaminar Approach for L4/5 and L5/S1 Two-Level Disc Herniation.Orthop Surg. 2021 May;13(3):979-988. doi: 10.1111/os.12862. Epub 2021 Apr 5. Orthop Surg. 2021. PMID: 33821557 Free PMC article.
-
Should adjacent asymptomatic lumbar disc herniation be simultaneously rectified? A retrospective cohort study of 371 cases that received an open fusion or endoscopic discectomy only on symptomatic segments.Spine J. 2021 Mar;21(3):411-417. doi: 10.1016/j.spinee.2020.09.003. Epub 2020 Sep 16. Spine J. 2021. PMID: 32947038
-
Adjuvant surgical decision-making system for lumbar intervertebral disc herniation after percutaneous endoscopic lumber discectomy: a retrospective nonlinear multiple logistic regression prediction model based on a large sample.Spine J. 2021 Dec;21(12):2035-2048. doi: 10.1016/j.spinee.2021.07.012. Epub 2021 Jul 20. Spine J. 2021. PMID: 34298160
-
Comparison of percutaneous endoscopic lumbar discectomy versus microendoscopic discectomy for the treatment of lumbar disc herniation: a meta-analysis.Int Orthop. 2019 Apr;43(4):923-937. doi: 10.1007/s00264-018-4253-8. Epub 2018 Dec 13. Int Orthop. 2019. PMID: 30547214
-
Percutaneous Endoscopic Lumbar Discectomy Versus Posterior Open Lumbar Microdiscectomy for the Treatment of Symptomatic Lumbar Disc Herniation: A Systemic Review and Meta-Analysis.World Neurosurg. 2018 Dec;120:352-362. doi: 10.1016/j.wneu.2018.08.236. Epub 2018 Sep 8. World Neurosurg. 2018. PMID: 30205219
Cited by
-
Predictive Factors for Residual Low Back Pain Following Percutaneous Endoscopic Lumbar Discectomy in Patients with Lumbar Disc Herniation.Med Sci Monit. 2024 Jan 6;30:e942231. doi: 10.12659/MSM.942231. Med Sci Monit. 2024. PMID: 38183217 Free PMC article.
-
Comparing mid-term outcomes and patient satisfaction between percutaneous endoscopic lumbar discectomy and microendoscopic discectomy for foraminal and extraforaminal lumbar disc herniations: a retrospective matched cohort study.Front Surg. 2025 Feb 19;12:1554970. doi: 10.3389/fsurg.2025.1554970. eCollection 2025. Front Surg. 2025. PMID: 40046499 Free PMC article.
-
[Sport after disc herniation].Orthopadie (Heidelb). 2024 Dec;53(12):928-934. doi: 10.1007/s00132-024-04580-w. Epub 2024 Nov 21. Orthopadie (Heidelb). 2024. PMID: 39570392 Review. German.
-
Effect of type 2 diabetes mellitus on patients undergoing percutaneous endoscopic lumbar discectomy: a retrospective propensity score-matched cohort study.Eur Spine J. 2025 Jun;34(6):2321-2328. doi: 10.1007/s00586-025-08808-x. Epub 2025 Mar 29. Eur Spine J. 2025. PMID: 40155440
References
-
- Kambin P, Sampson S. Posterolateral percutaneous suction-excision of herniated lumbar intervertebral discs. Report of interim results. Clin Orthop Relat Res. 1986;(207):37–43. - PubMed
-
- Gadjradj PS, Harhangi BS. Full-endoscopic transforaminal discectomy versus open microdiscectomy for sciatica: Update of a systematic review and meta-analysis. Spine (Phila Pa 1976) 2022;47(18):E591–E94. - PubMed
-
- Choi KC, Lee JH, Kim JS, et al. Unsuccessful percutaneous endoscopic lumbar discectomy: A single-center experience of 10,228 cases. Neurosurgery. 2015;76(4):372–81. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
