

Amyloid Transthyretin Cardiomyopathy in Elderly Patients With Aortic Stenosis Undergoing Transcatheter Aortic Valve Implantation
- PMID: 37581394
- PMCID: PMC10492930
- DOI: 10.1161/JAHA.123.030271
Amyloid Transthyretin Cardiomyopathy in Elderly Patients With Aortic Stenosis Undergoing Transcatheter Aortic Valve Implantation
Abstract
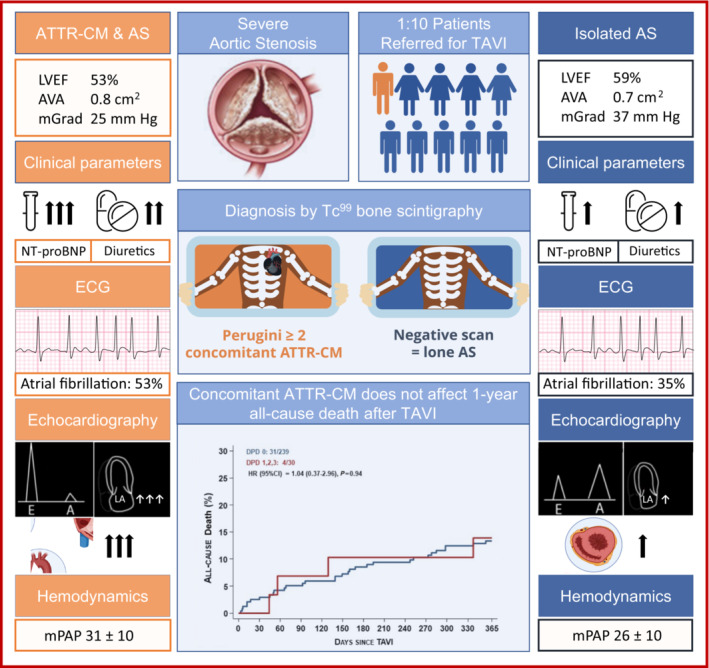
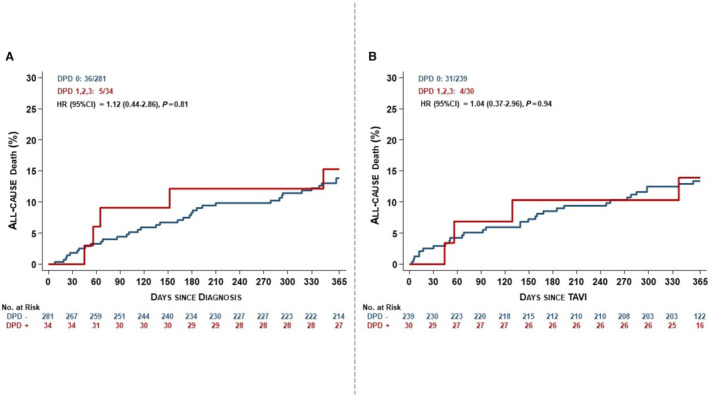
Background The prevalence of calcific aortic stenosis and amyloid transthyretin cardiomyopathy (ATTR-CM) increase with age, and they often coexist. The objective was to determine the prevalence of ATTR-CM in patients with severe aortic stenosis and evaluate differences in presentations and outcomes of patients with concomitant ATTR-CM undergoing transcatheter aortic valve implantation. Methods and Results Prospective screening for ATTR-CM with Technetium99-3,3-diphosphono-1,2-propanodicarboxylic acid bone scintigraphy was performed in 315 patients referred with severe aortic stenosis between August 2019 and August 2021. Myocardial Technetium99-3,3-diphosphono-1,2-propanodicarboxylic acid tracer uptake was detected in 34 patients (10.8%), leading to a diagnosis of ATTR-CM in 30 patients (Perugini ≥2: 9.5%). Age (85.7±4.9 versus 82.8±4.5; P=0.001), male sex (82.4% versus 57.7%; P=0.005), and prior carpal tunnel surgery (17.6% versus 4.3%; P=0.007) were associated with coexisting ATTR-CM, as were ECG (discordant QRS voltage to left ventricular wall thickness [42% versus 12%; P<0.001]), echocardiographic (left ventricular ejection fraction 48.8±12.8 versus 58.4±10.8; P<0.001; left ventricular mass index, 144.4±45.8 versus 117.2±34.4g/m2; P<0.001), and hemodynamic parameters (mean aortic valve gradient, 23.4±12.6 versus 35.5±16.6; P<0.001; mean pulmonary artery pressure, 29.5±9.7 versus 25.8±9.5; P=0.037). Periprocedural (cardiovascular death: hazard ratio [HR], 0.71 [95% CI, 0.04-12.53]; stroke: HR, 0.46 [95% CI, 0.03-7.77]; pacemaker implantation: HR, 1.54 [95% CI, 0.69-3.43]) and 1-year clinical outcomes (cardiovascular death: HR, 1.04 [95% CI, 0.37-2.96]; stroke: HR, 0.34 [95% CI, 0.02-5.63]; pacemaker implantation: HR, 1.50 [95% CI, 0.67-3.34]) were similar between groups. Conclusions Coexisting ATTR-CM was observed in every 10th elderly patient with severe aortic stenosis referred for therapy. While patients with coexisting pathologies differ in clinical presentation and echocardiographic and hemodynamic parameters, peri-interventional risk and early clinical outcomes were comparable up to 1 year after transcatheter aortic valve implantation. REGISTRATION URL: https://www.clinicaltrials.gov. Unique identifier: NCT04061213.
Keywords: 99mTc‐DPD scintigraphy; TAVI; aortic stenosis; cardiac amyloidosis; transthyretin.
Figures

References
-
- Yadgir S, Johnson CO, Aboyans V, Adebayo OM, Adedoyin RA, Afarideh M, Alahdab F, Alashi A, Alipour V, Arabloo J, et al. Global, regional, and national burden of calcific aortic valve and degenerative mitral valve diseases, 1990‐2017. Circulation. 2020;141:1670–1680. doi: 10.1161/CIRCULATIONAHA.119.043391 - DOI - PubMed
-
- Tanskanen M, Peuralinna T, Polvikoski T, Notkola IL, Sulkava R, Hardy J, Singleton A, Kiuru‐Enari S, Paetau A, Tienari PJ, et al. Senile systemic amyloidosis affects 25% of the very aged and associates with genetic variation in alpha2‐macroglobulin and tau: a population‐based autopsy study. Ann Med. 2008;40:232–239. doi: 10.1080/07853890701842988 - DOI - PubMed
-
- Gonzalez‐Lopez E, Gallego‐Delgado M, Guzzo‐Merello G, de Haro‐Del Moral FJ, Cobo‐Marcos M, Robles C, Bornstein B, Salas C, Lara‐Pezzi E, Alonso‐Pulpon L, et al. Wild‐type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur Heart J. 2015;36:2585–2594. doi: 10.1093/eurheartj/ehv338 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
